

Retinopathy of prematurity (ROP) is a proliferative retinal vascular disease that develops in premature infants [1,2]. The incidence of childhood blindness due to ROP ranges from 3% to 10% worldwide [3,4,5,6]. Normal retinal vascular growth and development are disrupted by fetal environmental changes. Physiological hyperoxia causes vascular endothelial growth factor (VEGF)-mediated cessation of retinal vascular development [2,7]. The release of VEGF also causes vitreoretinal neovascularization, which leads to retinal traction, detachment, and hemorrhage, with profound loss of visual function [8,9,10].
Early detection and appropriately-timed intervention are critical to treatment and long-term outcomes of this disease [11,12,13]. Current treatment strategies include early treatment with laser photocoagulation based on the 2004 Early Treatment for Retinopathy of Prematurity study [14], or with intravitreal anti-VEGF injections, based on groundbreaking studies such as the 2011 Bevacizumab Eliminates the Angiogenic Threat ROP study [12], either alone or in combination [15,16]. Although there are many benefits to anti-VEGF therapy, several studies have found temporary systemic suppression of VEGF and other growth factors after intravitreal injection in neonatal infants [17,18], triggering concern regarding potential neurological or developmental delays [19].
One particularly concerning long-term consequence of ROP treatment is the elevated rate of myopia and high myopia in these infants, especially with the already high prevalence in Korean and Japanese populations [20]. Although several studies have noted greater prevalence and severity of myopia in laser-treated eyes over anti-VEGF, there are striking limitations due to the wide range of ages at refraction and variation in treatment zone, which were not always taken into account [21,22].
Therefore, in this study we examined the long-term refractive outcomes of infants treated for ROP by collecting a large number of cases and adjusting for age at the time of refraction in analysis. We also noted the rate of recurrence and the incidence of systemic complications.
Materials and Methods
This retrospective case study was performed at two tertiary referral-based hospitals, Severance Hospital and Gangnam Severance Hospital, which are affiliated with Yonsei University College of Medicine. Consecutive infants diagnosed with ROP and treated from August 2006 to December 2013 were included, and their medical charts were reviewed. This study was conducted with institutional review board approval from Gangnam Severance Hospital (3-2018-0050) and adhered to the tenets of the Declaration of Helsinki. Informed consent was obtained from the parents or guardians of all subjects.
Infants were screened for ROP if they were born at gestational age <32 weeks and their birthweight was <1,500 g; more mature and larger infants were examined if the clinical course was complex and/or unstable, as determined by the primary neonatologist. All ophthalmic examinations were performed by qualified ophthalmologists using the revised guidelines of the 2005 International Committee for the Classification of ROP to determine the stage and zone [23]. The indications for treatment were infants who met the criteria for type 1 ROP used in the Early Treatment for Retinopathy of Prematurity study [14], although earlier treatment was performed at the primary ophthalmologists' discretion in cases involving signs of clinical pre-plus disease, which was defined as abnormal vascular changes insufficient for the diagnosis of plus disease.
For laser photocoagulation, infants were treated under general anesthesia using an indirect diode laser system with a handheld aspheric lens using scleral depression. For anti-VEGF injection, either bevacizumab (0.625 mg/0.025 mL; off-label Avastin, Genentech, San Francisco, CA, USA) or ranibizumab (0.2 mg/0.02 mL; Lucentis, Novartis, Basel, Switzerland) [18,24] was injected into the diseased eye aseptically at the pars plana, 0.5 to 1 mm posterior to the limbus, using a sterile 30-gauge needle. The patients were re-examined the next day and then every week to monitor disease progression. Dilated fundus examinations were performed with indentation indirect ophthalmoscopy at every visit to confirm disease regression and vascularization up to the ora serrata.
All infants underwent regular follow-up visits and eye examination including initial cycloplegic retinoscopy or subsequent manifest refraction by certified ophthalmologists. If hyperopia was noted at the initial cycloplegic refraction, subsequent examinations were done with cycloplegic refraction. The spherical and cylinder power, as well as the spherical equivalent (SE) are all noted in diopters (D). Patients who underwent vitrectomy or scleral buckling due to retinal detachment (five eyes from three patients), who underwent both laser and anti-VEGF injection (five eyes from three patients), or who lacked refraction data (54 eyes from 28 patients) were excluded.
The patients were grouped according to the type of treatment received: intravitreal anti-VEGF or laser photocoagulation. The main outcome was long-term refractive error measured at the age of 4 years. Secondary outcomes included recurrence rate and treatment complications.
Statistical analyses were performed using Stata ver. 13.1 (Stata Corp., College Station, TX, USA). Values are expressed as mean ┬▒ standard deviation, with ranges given when appropriate. Chi-square test (Fisher exact test) and analysis of variance were used to compare the two treatment groups. A generalized estimating equation was used to compare refractive error between groups. Generalized estimating equation models that accounted for age at the time of refractive error measurement and within-patient inter-eye correlations were used to compare SE between the two treatment groups. Clustered regression analysis was used with each individual representing one cluster to consider similar characteristics between the right and left eyes in a single child and was performed to assess the impact of various factors on refractive outcomes. A p-value less than 0.05 was considered statistically significant.
Results
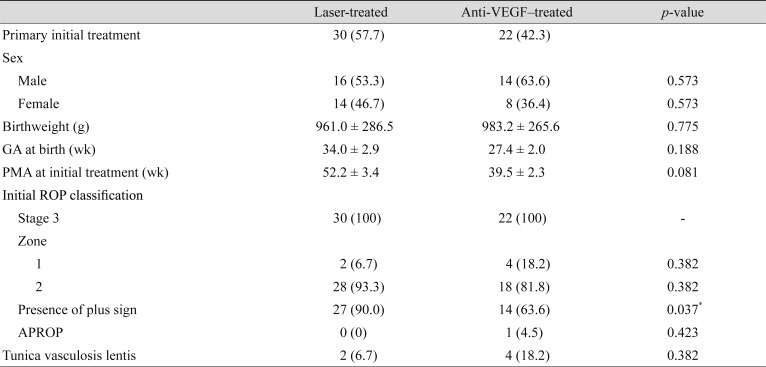
Refractions were available for 27 of 55 (49.1%) eligible patients. The baseline characteristics of each treatment group are summarized in Table 1. A total of 30 eyes (15 subjects) were treated with laser and 22 eyes (12 subjects) with anti-VEGF. In the anti-VEGF group, 20 (90.9%) eyes were treated with bevacizumab and 2 (9.1%) with ranibizumab. There were no significant differences between the two groups in sex ratio, gestational age, birthweight, post-menstrual age at treatment, and ROP stage/zone distribution. The mean age at refraction was 4.7 ┬▒ 0.3 years for the laser group and 4.4 ┬▒ 0.3 years for the anti-VEGF group.
Refractive outcomes
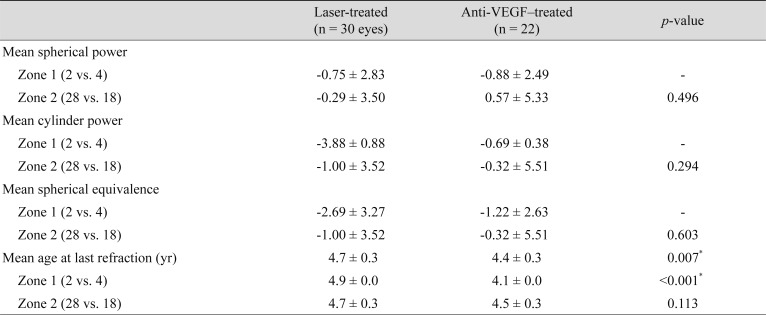
Refractive error grouped according to the treatment zone is summarized in Table 2. No significance was noted in mean SE between treatment groups (ŌłÆ1.0 D in the laser group vs. ŌłÆ0.3 D in the anti-VEGF group, p = 0.603). Similarly, no differences were found in mean spherical or cylinder power.
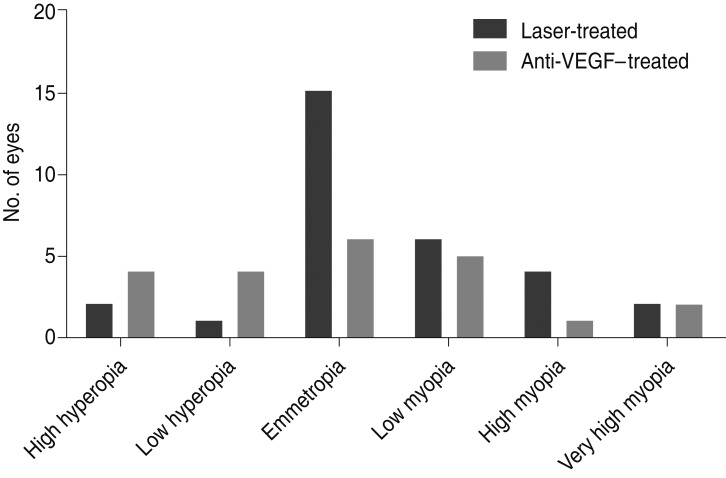
The distribution of refractive outcomes, categorized as high hyperopia to very high myopia, can be seen in Fig. 1. These refractive categories were chosen based on previous studies [25,26]. There were no significant differences in the distribution between the two groups. When combining all myopia (ŌēźŌłÆ1 D), there were 11 eyes (36.7%) in the laser group and 8 (36.4%) in the injection group, which was not a significant difference (p = 0.607). Additionally, no differences in the prevalence of myopia between the treatment groups were found when grouped according to the treatment zones.
Clustered regression analysis revealed that only gestational age showed significant correlation with the mean SE (p < 0.001; 95% confidence interval, ŌłÆ0.007 to ŌłÆ0.002). Other factors such as the treatment type, ROP treatment zone, and birthweight were not significant factors.
Complications and recurrences
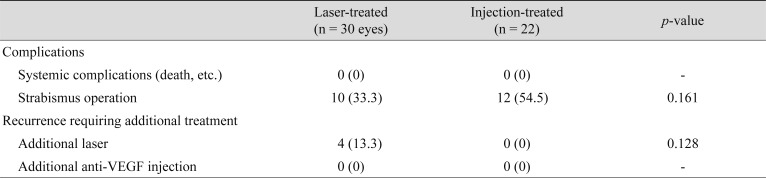
Systemic complications and recurrences requiring additional treatment can be found in Table 3. No systemic complications were reported in either treatment group. The rate of recurrences requiring additional treatment was 13.3% (n = 4) for the laser group and 0% (n = 0) for the anti-VEGF group (p = 0.128). Fully vascularized retinas to the ora serrata were noted in 22 (100%) eyes in the anti-VEGF group.
Discussion
Despite a recent trend in treating ROP primarily with intravitreal anti-VEGF injections, due in part to potential systemic complications, a large proportion of infants are still treated via laser therapy [27,28]. Owing to several studies reporting an association between myopia and laser treatment, concern regarding long-term refractive outcomes may influence primary ophthalmologists' recommendations regarding treatment method [25,29]. In our study, we found that in children aged 4 years, the type of treatment (laser or injection) did not appear to influence long-term refractive outcomes of ROP.
Conflicting results have been reported in a few studies regarding the long-term refractive outcomes of ROP treatment [30], with major limitations acknowledged due to the wide range of ages and low number of cases involved. A literature review by Aghdam et al. [20] in 2016 found that mean final refractive error in 9 studies ranged from ŌłÆ4.4 to ŌłÆ10.1 D in laser-treated eyes and +0.4 to ŌłÆ3.7 D in injection-treated eyes, only one study reporting that outcomes were similar. However, age at the time of refraction ranged from 7 to 76 months with potential observer bias and small sample sizes, which made drawing definitive conclusions difficult. In our study of children aged 4 years, we noted no statistically significant differences in spherical/cylinder power and calculated SE between laser- or anti-VEGF-treated eyes.
When we compared the effects of treatment zones in the development of myopia, we noted that there was an overall trend toward more severe myopia in eyes treated closer to the posterior pole (zone 1 vs. zone 2), which varies from a previous report where no difference in myopia severity was noted between zone 1 and posterior zone 2 ROP [25]. Unfortunately, the number of cases treated in Zone 1 in our study was too small to draw meaningful statistical conclusions. Additionally, we noted no statistically significant differences when myopia severity was compared between laser and anti-VEGF in each treatment zone. Thus, our results suggest that the greater proportion of myopia noted in children treated for ROP is an outcome intrinsic to the disease [31], and not necessarily influenced by type of treatment.
In terms of safety, we found no reports of systemic complications such as neurodevelopmental delay or death in either treatment group. The recurrence rate was 0% for laser- and 13.3% for anti-VEGF-treated eyes, which is low compared to previously published studies with rates ranging from 13% to 35.4% [32,33,34]. In cases with zone 2 or 3 ROP, laser therapy appears to be a viable treatment option due to its lower rate of recurrence, especially in cases in which timely follow-up is difficult or there may be low compliance to additional therapies. However, the anti-VEGF group was observed to have fully vascularized retinas up to the ora serrata in 100% of eyes on the most recent follow-up.
This study has several limitations. First, it was a retrospective study with a variable follow-up period and without appropriate controls, such as those for treatment indications that might call for earlier treatment for type 1 ROP. Second, our study population was limited to Asian patients in a tertiary university hospital setting. Third, not all systemic complications may have been properly observed or reported to us from the neonatologists. Finally, we did not routinely perform fluorescein angiography to document fully vascularized retinas in these children; however, a retina specialist performed thorough fundus examination at each follow-up outpatient visit. The strengths of this study include statistical comparison of long-term refractive outcomes of similarly-aged children treated at two affiliated institutions using the same treatment protocols.
In conclusion, our study demonstrated that long-term refractive outcomes in infants treated for ROP did not vary between laser and anti-VEGF injection treatment groups. Concern regarding refractive outcome should not be the most important factor when selecting treatment modality. Considering the low rate of recurrence and established safety, conventional laser therapy remains a viable primary therapeutic option in select cases.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






