Vitrectomy Combined with Intravitreal Triamcinolone Acetonide Injection and Macular Laser Photocoagulation for Nontractional Diabetic Macular Edema
Article information
Abstract
Purpose
To evaluate the efficacy of vitrectomy combined with intravitreal injection of triamcinolone acetonide (IVTA) and macular laser photocoagulation for the treatment of nontractional diabetic macular edema (DME) refractory to anti-vascular endothelial growth factor (VEGF) therapy.
Methods
Twenty-eight eyes from 28 subjects who were diagnosed with nontractional DME refractory to three or more sequential anti-VEGF injections underwent sequential vitrectomy, IVTA, and macular laser photocoagulation. Changes in best-corrected visual acuity (BCVA) and central subfield thickness (CST) during the six months following vitrectomy were evaluated. Additionally, the CST and BCVA outcomes were compared with those of 26 eyes treated with the same triple therapy for nontractional DME refractory to conventional treatment, such as IVTA or macular laser photocoagulation, or both.
Results
The mean logarithm of the minimum angle of resolution BCVAs before and one, three, and six months after vitrectomy were 0.44 ± 0.15, 0.36 ± 0.18, 0.31 ± 0.14, and 0.34 ± 0.22, respectively. The mean CSTs were 433.3 ± 77.9, 329.9 ± 59.4, 307.2 ± 60.2, and 310.1 ± 80.1 microns, respectively. The values of both BCVA and CST at one, three, and six months were significantly improved from baseline (p < 0.05). The extent of CST reduction during the first month after triple therapy was greater in eyes refractory to conventional treatment than in eyes refractory to anti-VEGF (p = 0.012).
Conclusions
Vitrectomy combined with IVTA and macular laser photocoagulation had a beneficial effect on both anatomical and functional outcomes in eyes with nontractional DME refractory to anti-VEGF therapy.
Diabetic macular edema (DME) is a common microvascular complication and the principle cause of visual impairment in patients with diabetes. In the past, the most widely used non-surgical treatments for DME included macular laser photocoagulation [1], intravitreal injection of triamcinolone acetonide (IVTA) [2-4], posterior sub-Tenon injection of triamcinolone acetonide (PSTA) [5,6], or a combination of these therapies [7,8].
Intravitreal injection of anti-vascular endothelial growth factor (VEGF) is a method that was recently developed for the treatment of retinal disorders related to ischemia. This therapy is highly effective in treating DME [9-14], and there is evidence that its efficacy is superior to that of conventional methods [11,12,14-16]. However, the results of recent case series show that macular edema persists in some patients despite multiple intravitreal anti-VEGF injections over a long treatment period [10-13].
Vitrectomy has been advocated for the treatment of DME refractory to non-surgical treatments [17-25]. Previous studies have demonstrated a significant decrease in macular thickness [17,18,20-23,25], but improvements in visual acuity following vitrectomy have been controversial [17-23,25]. The postulated mechanisms of action of vitrectomy include the removal of possible sources of traction [18,22,26]; improving transvitreal oxygenation of the retina [27]; removal of the posterior hyaloids, which harbor vasopermeable factors [28]; and removal of condensed chemical mediators that promote vascular permeability [17,20,21]. Although vitrectomy is beneficial in DMEs refractory to conventional non-surgical therapies, the outcomes of vitrectomy for DME refractory to anti-VEGF could be different.
Although the outcomes of vitrectomy in the era of anti-VEGF therapy have been investigated [29,30], most of the patients in these studies were treated with macular laser photocoagulation, IVTA, or PSTA prior to vitrectomy. The outcome of vitrectomy for DME refractory to anti-VEGF therapy remains to be fully elucidated.
Previously, we reported the effect of vitrectomy combined with IVTA and macular laser photocoagulation for DME refractory to conventional treatment such as macular laser photocoagulation [31]. The primary objective of the current study was to evaluate the efficacy of a triple therapy for the treatment of nontractional DME refractory to anti-VEGF therapy (anti-VEGF group). In addition, we compared the outcomes of vitrectomy between DME refractory to anti-VEGF therapy and DME refractory to conventional macular laser photocoagulation, corticosteroid therapy, or both (conventional treatment group).
Materials and Methods
This retrospective study was performed at a single center and adhered to the tenets of the Declaration of Helsinki. The study was approved by the institutional review board (no. 2011-07-102).
Patients
The study sample included patients who underwent sequential combined therapy involving vitrectomy, IVTA, and macular laser photocoagulation between September 2007 and September 2009 as treatment for nontractional DME refractory to anti-VEGF treatments. Intractable DME was defined as biomicroscopically, angiographically, and tomographically confirmed diffuse DME that had a central subfield thickness (CST) of 300 microns or more despite three or more serial intravitreal injections of bevacizumab (1.25 mg in 0.05 mL for each injection). Major exclusion criteria included 1) combined cataract extraction with vitrectomy, 2) active proliferative diabetic retinopathy, 3) uncontrolled intraocular pressure (IOP), 4) prior history of vitreoretinal surgery, 5) evidence of any retinal disease that might affect visual acuity or macular microstructure, and 6) less than six months of follow-up after vitrectomy. When both eyes met the inclusion criteria, the one that had undergone prior surgery was included. Data from patients who underwent the same therapy between September 2006 and September 2008 for nontractional DME refractory to conventional macular focal laser photocoagulation, corticosteroid therapy, or both were also collected according to the same inclusion and exclusion criteria in order to make a comparison of outcomes.
Preoperative examinations
Preoperative ocular examinations included best-corrected visual acuity (BCVA) using Snellen visual acuity charts, tonometry, slit-lamp biomicroscopy, and fundus examination. Optical coherence tomography (OCT) was conducted in each eye using the Zeiss Stratus OCT system (Carl Zeiss Meditec, Dublin, CA, USA) in order to evaluate abnormalities of the vitreomacular interface and to determine the macular thickness. The fast macular thickness map protocol with 6-mm radial lines consisting of 128 A-scans per line was used in the study. The thickness of the innermost concentric circle with a diameter of 1.0 mm was defined as the CST. Fluorescein angiograms and fundus photographs were also obtained. The presence of subfoveal hard exudates was evaluated based on preoperative fundus photographs.
Surgical procedure
Triple therapy involving vitrectomy, IVTA, and macular laser photocoagulation was sequentially administered according to the method described in our previous report [31]. Vitrectomy with removal of the internal limiting membrane (ILM) was conducted in all of the patients. The ILM was peeled off from a round area with a diameter of approximately 2 disc diameters centered on the fovea. In most cases, the ILM was removed without the assistance of staining dye. Panretinal endolaser photocoagulation coupled with vitrectomy was performed in cases with extensive retinal capillary dropout or with apparent high-risk characteristics. At the conclusion of the operation, triamcinolone acetonide (4 mg in 0.1 mL) was injected intravitreally. All patients were instructed to maintain a sitting position for approximately six hours in the immediate postoperative period to facilitate inferior sedimentation of the injected triamcinolone acetonide. Direct and grid macular laser photocoagulation was conducted two weeks after vitrectomy. The preoperative fluorescein angiography and the topographic map of macular thickness facilitated the identification of the macular area to be treated by laser photocoagulation. The diffusely thickened macular area identified from the topographic map before surgery was treated with grid pattern photocoagulation, and leaking microaneurysms identified via fluorescein angiography were treated with direct laser photocoagulation.
Postoperative examination
Postoperative examination, including slit-lamp biomicroscopy, applanation tonometry, and fundus examinations, were conducted two days, one week, and one month after vitrectomy, and subsequent examinations were generally scheduled every one to three months.
As outcome measures, BCVA and CST were recorded at one, three, and six months after the administration of triple therapy. The BCVA was then transformed to a logarithmic scale for statistical analysis. Additionally, we compared the changes in BCVA and CST after triple therapy between the anti-VEGF group and the conventional treatment group for the defined perioperative periods (preoperatively to 1 month postoperatively, between one to three months postoperatively, and between three to six months postoperatively).
Statistical analysis
Statistical analyses were performed using a commercially available statistical package (SPSS ver. 18.0; SPSS Sciences, Chicago, IL, USA). The data were analyzed using repeated-measures analysis of variances with Bonferroni's correction. Comparisons between the anti-VEGF group and the conventional treatment group were performed using an independent samples t-test with Bonferroni's correction. Baseline characteristics were compared between the anti-VEGF group and the conventional treatment group using the independent sample t-test, the chi-square test, and Fisher's exact test. A p-value of less than 0.05 was considered significant.
Results
Forty-two eyes of 42 subjects with DME refractory to anti-VEGF therapy underwent treatment and completed at least six months of follow-up, and 28 were included in the analysis. The other 14 patients were excluded from the study for the following reasons: 1) combined cataract extraction with vitrectomy (nine patients), 2) active proliferative diabetic retinopathy (two patients), 3) prior history of vitreoretinal surgery (one patient), 4) evidence of any retinal disease that might affect visual acuity or macular microstructure (two patients). No patient required additional procedures for DME or cataract extraction during the six-month postoperative follow-up period.
The mean age of the included patients was 58.1 ± 12.5 years (mean ± standard deviation), and 53.6% (15 of 28) of the subjects were male. The mean duration of diabetes was 13.4 ± 6.9 years. Subfoveal hard exudates were detected in seven eyes (25.0%). Eleven eyes (39.3%) had undergone macular laser photocoagulation, corticosteroid therapy, or both prior to intravitreal bevacizumab injection. The study eyes had undergone serial intravitreal bevacizumab injection a mean of 3.8 ± 1.4 times (3 to 8 times) with four to six week intervals between each injection before the surgery. The mean period between the last intravitreal bevacizumab injection and vitrectomy was 4.4 ± 1.6 months. Eight eyes (28.6%) were pseudophakic before surgery. The baseline characteristics of the patients are presented in Table 1.
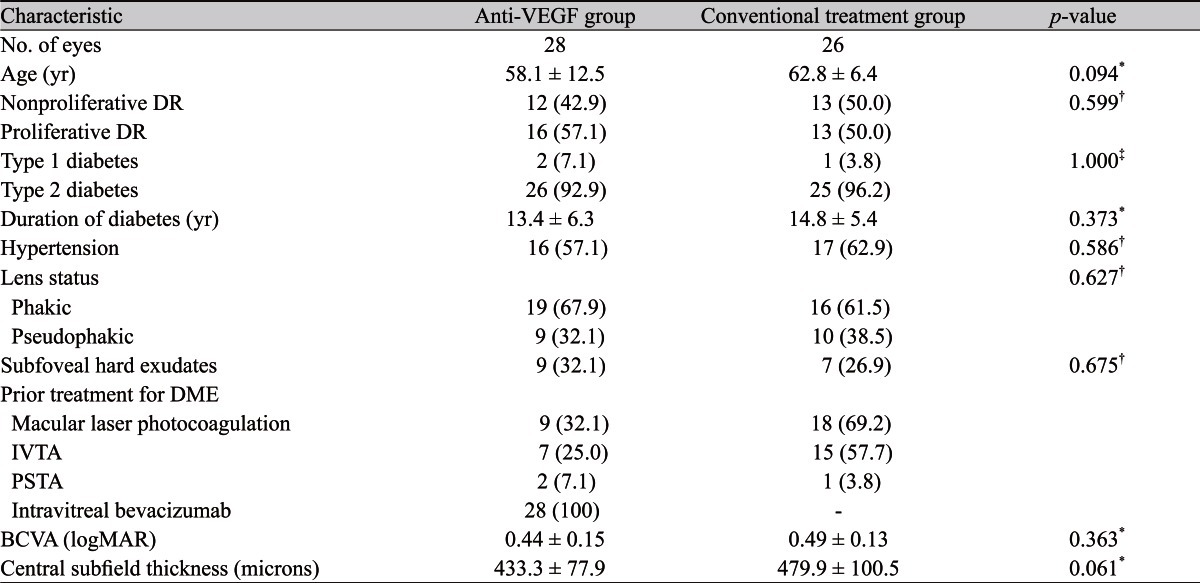
Baseline characteristics of patients with DME refractory to anti-VEGF group and refractory to intravitreal triamcinolone therapy or macular laser photocoagulation (conventional treatment group)
Treatment outcomes in eyes with diabetic macular edema refractory to anti-vascular endothelial growth factor therapy
Changes in the mean BCVA after triple therapy are shown in Fig. 1. The mean logarithm of the minimal angle of resolution (logMAR) BCVA values were 0.44 ± 0.15, 0.36 ± 0.18, 0.31 ± 0.14, and 0.34 ± 0.22 before surgery and at one, three, and six months after vitrectomy, respectively. Compared with the preoperative value, BCVA improved significantly one, three, and six months after vitrectomy (p < 0.001, p < 0.001, and p = 0.009, respectively). Compared to the preoperative value, eight (28.6%) and seven (25.0%) eyes showed two or more logMAR lines of improvement in visual acuity at the three-month and six-month postoperative examinations, respectively.
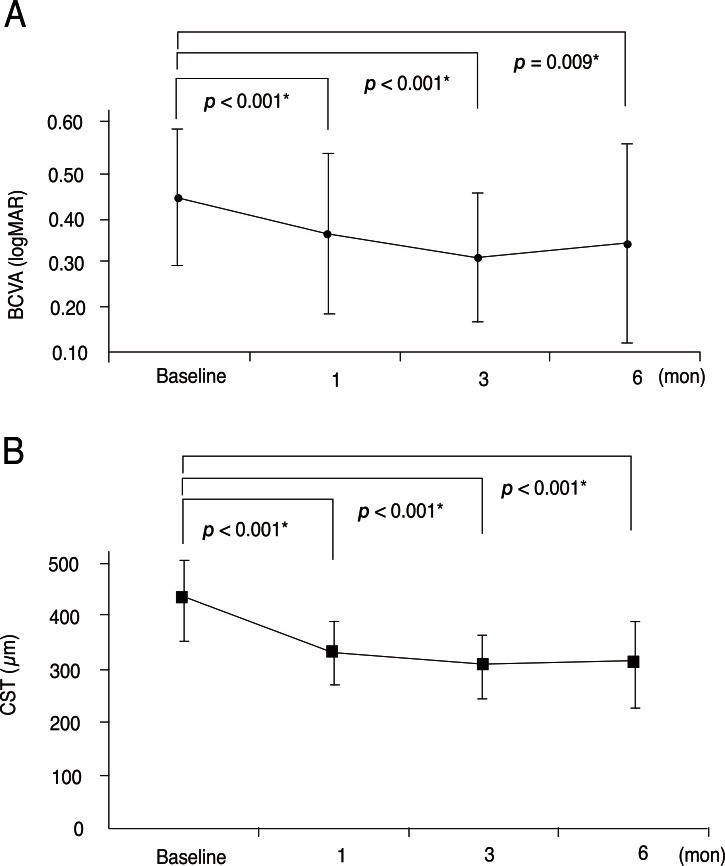
Graph illustrating changes in the logarithm of the minimal angle of resolution (logMAR) best-corrected visual acuity (BCVA, A), and the central subfield thickness (CST, B) at baseline and one, three, and six months after sequential combined vitrectomy, intravitreal triamcinolone acetonide, and macular laser photocoagulation for the treatment of diabetic macular edema between eyes refractory to anti-vascular endothelial growth factor. Statistical significance was determined using repeated measures analysis of variance. Asterisks indicate statistically signif icant results after Bonferroni's correction. Cataract extraction was not conducted during the study period.
Changes in the mean CST after triple therapy are also shown in Fig. 1. The mean CST was 433.3 ± 77.9, 329.9 ± 59.4, 307.2 ± 60.2, and 310.1 ± 80.1 microns before surgery and at one, three, and six months after vitrectomy, respectively. Compared with the preoperative value, the CST decreased significantly at one, three, and six months after vitrectomy (p < 0.001, p < 0.001, and p < 0.001, respectively). The mean CST showed a tendency to decline during the first three months after vitrectomy, but increased slightly between the three- and six-month postoperative examinations. At three months, 22 (78.6%) and 19 (67.9%) eyes had 50- and 100-micron or more decreases in thickness from baseline, respectively. At six months, 21 (75.0%) and 17 (60.7%) eyes had 50- and 100-micron or more decreases in thickness from baseline, respectively.
Cataract development or progression was detected in 7 of 19 phakic eyes (36.8%). No patients underwent cataract extraction during the six-month follow-up period. A postoperative increase in IOP was noted in four eyes (14.3%), and was successfully treated with anti-glaucoma medication. There were no severe postoperative complications such as retinal detachment, iris neovascularization, or endophthalmitis.
Comparison between the anti-vascular endothelial growth factor group and the conventional treatment group
Twenty-six eyes from 26 patients were included in the conventional treatment group. The baseline characteristics, including mean age, severity of diabetic retinopathy, duration of diabetes, presence of hypertension, lens status, and preoperative BCVA, were not different compared to the anti-VEGF therapy group (Table 1). Although the preoperative CST was slightly larger in the conventional treatment group, the difference was not significant (p = 0.062). In the conventional treatment eyes, the mean logMAR BCVA values were 0.47 ± 0.13, 0.40 ± 0.19, 0.35 ± 0.15, and 0.41 ± 0.22 before surgery and at one, three, and six months after vitrectomy, respectively. The mean CSTs were 479.9 ± 100.5, 310.6 ± 55.9, 295.9 ± 73.6, and 291.1 ± 72.5 before surgery and at one, three, and six months after vitrectomy, respectively. Table 2 shows comparisons of the amount of change in CST and BCVA during the postoperative period between the anti-VEGF group and the conventional treatment group. The changes in BCVA between the preoperative visit and one month postoperatively, one month and three months postoperatively, and three months and six months postoperatively were not significant between the two groups (p = 0.790, p = 0.654, and p = 0.339, respectively). In addition, the amount of change in CST in the periods between one to three months postoperatively and three to six months postoperatively were not significant between the two groups (p = 0.250, p = 0.650, respectively). However, the conventional treatment group showed a significantly greater reduction in CST during the first month after vitrectomy (p = 0.012), and this difference was significant after Bonferroni's correction. Although cataract development or progression was detected in 7 of 16 phakic eyes (43.8%), no patients underwent cataract extraction during the six-month postoperative follow-up period. A postoperative increase in IOP was noted in three eyes (11.5%), and was successfully treated with anti-glaucoma medication.
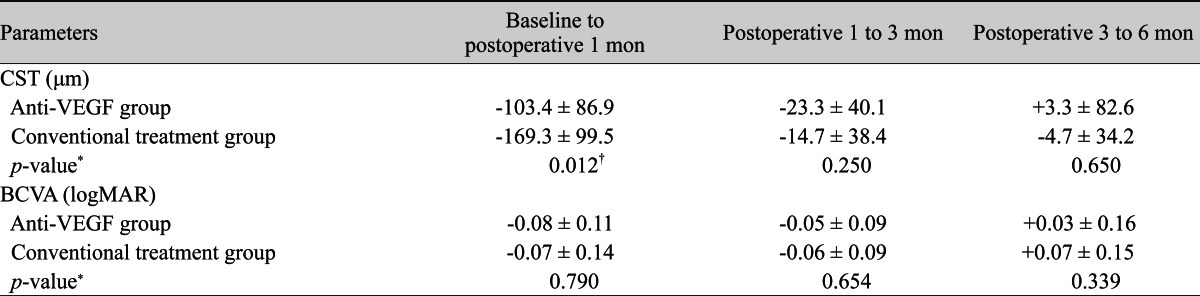
Comparison of the changes in CST and BCVA after triple therapy between anti-VEGF group and conventional treatment group
Discussion
In this study, CST was markedly reduced and visual acuity was significantly improved after triple therapy in eyes refractory to prior anti-VEGF therapy. The prominent reduction in CST was the most remarkable finding of this study. To avoid the possible influence of pseudophakic macular edema on CST, we excluded all eyes that underwent combined cataract extraction. Thus, the efficacy of the treatment for reducing CST was accurately estimated despite some influence of cataract development or progression, which cannot be avoided when estimating visual acuity outcomes. The mean CST at 6 months was 310 microns, which is still thicker than normal values. This result suggests the limited efficacy of this triple therapy. Compared to the preoperative value, however, CST was significantly decreased throughout the six-month follow-up period. Eventually, more than half of the eyes experienced a 100-micron or more reduction in CST after six months of follow-up. Additionally, BCVA improved significantly during the six-month follow-up period. A slight deterioration in mean BCVA was noted between three and six months postoperatively; however, we believe that nucleosclerotic cataract development or progression rather than recurrence of DME was mainly responsible for this deterioration. The BCVA measured at six months postoperatively was still significantly better than the baseline value. Both the CST and BCVA outcomes in this study strongly indicate that vitrectomy combined with IVTA and macular laser photocoagulation is a useful therapeutic modality for refractory DME, even in the era of anti-VEGF therapy.
Approximately one-thirds of the eyes in the anti-VEGF group were also refractory to other treatments, including macular laser photocoagulation, corticosteroid therapy, or both. In these eyes, DME was not merely refractory to anti-VEGF therapy alone. However, we think this heterogeneity of prior treatments in our patients may reflect the real-world population because many clinicians generally try several different non-surgical methods before they decide to perform vitrectomy for refractory DME.
In our previous clinical trial, vitrectomy combined with IVTA and macular laser photocoagulation reduced macular thickness and improved visual outcomes in eyes with DME refractory to conventional laser or corticosteroid treatments [31]. The efficacy of this treatment was maintained for six months in the majority of eyes without additional treatment for DME. In addition, in our experience, the effect of triple therapy is maintained in many eyes for three years after treatment. We postulate the mechanism of action of triple therapy to be an increased supply of oxygen to the inner retina due to vitrectomy and reduced macular oxygen consumption as a result of macular laser photocoagulation, which is facilitated by IVTA. The triple therapy modalities may function in a synergistic manner to attenuate hypoxia in the inner foveal layers [31].
In two recent studies from the Diabetic Retinopathy Clinical Research Network (DRCR.net) that included patients with and without vitreomacular interface abnormality, vitrectomy was found to be beneficial with regard to reducing CMT [29,30]. However, the efficacy of improving visual acuity was limited. The CMT outcomes of our patients who were refractory to anti-VEGF therapy were comparable to the results of these two studies. However, we observed a more favorable visual acuity outcome in our patients. Although recent studies from DRCR.net have not identified long-term visual benefits, an improvement in visual acuity was noted during the first several months after IVTA [16,32]. In addition, improved visual acuity was noted in pseudophakic eyes for up to two years after IVTA plus macular laser photocoagulation [16]. Thus, we believe that the encouraging visual outcomes in our patients during the six-month follow-up period can be attributed to vitrectomy as well as combined IVTA and macular laser photocoagulation. In addition, the baseline characteristics of patients may have partially influenced the differences in visual outcomes. Compared to previous studies [29,30], a relatively small proportion of patients had type 1 diabetes, and the mean duration of diabetes was approximately seven years shorter in this study. A previous study demonstrated that the presence of subfoveal hard exudates is strongly associated with poor visual outcome after vitrectomy [19]. In this study, subfoveal hard exudates were detected on preoperative fundus photographs in approximately one-third of our patients. This proportion was similar to that reported in a study by Kumagai et al. [19], in which significant improvements in visual acuity after vitrectomy for nontractional DME were observed.
The pathogenesis of DME is a complicated process related to various cytokines [33-36]. Although recent studies showing the excellent efficacy of anti-VEGF therapy strongly indicate that VEGF is a very important causative agent of DME, investigators have also demonstrated the limited efficacy of single intravitreal anti-VEGF injection [37,38] and have highlighted the importance of other cytokines, such as IL-6 or ICAM-1, which cannot be suppressed by anti-VEGF agents [38]. The development of DME in our series of patients who were refractory to multiple intravitreal anti-VEGF injections might be more closely associated with other mechanisms rather than a VEGF-related mechanism. Thus, we postulated that the result of vitrectomy in DME patients refractory to anti-VEGF therapy might be different from previous studies that were conducted before anti-VEGF therapy became widely used for DME, and we conducted a comparison of treatment outcomes between an anti-VEGF group and a conventional treatment group.
We observed comparable anatomic and visual outcomes after triple therapy between the two groups. However, we found a difference in early postoperative CST outcomes between the anti-VEGF group and the conventional treatment group. The extent of the decrease in CST during the first postoperative year was greater, by approximately 66 microns, in the conventional treatment group. The extent of CST decrease following vitrectomy showed a positive correlation with preoperative CST [29], and the difference in CST outcomes in our study could be influenced by the larger initial CST values in the conventional treatment group. However, the initial difference was only 47 microns and was not significant. Thus, we suspect this difference in CST outcome was caused primarily by the differing efficacy of scavenging VEGF by vitrectomy between the two groups. The effect of several possible mechanisms of action of vitrectomy with regard to VEGF, such as removal of the posterior hyaloids, which harbor vasopermeable factors [28], and the removal of condensed VEGF, which promotes vascular permeability [17,20,21], might be diminished in DME refractory to anti-VEGF therapy. It is possible that DME refractory to intravitreal anti-VEGF therapy was caused partially by formation of VEGF from an ischemic retina. Because we performed panretinal endolaser photocoagulation in cases with extensive retinal capillary dropout or with apparent high-risk characteristics, resolution of DME after triple therapy may be partially attributable to ablation of the ischemic retina. The effect of panretinal photocoagulation on DME refractory to anti-VEGF therapy needs further investigation.
In this study, the ILM was removed in all patients. ILM removal was suggested to have a role in the resolution of nontractional DME by eliminating tangential traction force [39] or by preventing possible vitreoretinal traction due to attachment between the ILM and the residual vitreous cortex [40].
In addition to its retrospective nature and relatively small sample size, our study had several limitations. There was no control group for the triple therapy. Considering the possible differences in efficacy between ranibizumab and bevacizumab in patients with DME [41], it is possible that the results of our study may not be valid in eyes refractory to other anti-VEGF agents, such as ranibizumab or pegatanib. After 2009, we routinely performed intravitreal anti-VEGF injection for patients with DME before they underwent surgical intervention. Thus, surgeries in the conventional group (from September 2006 through September 2008) were usually performed in an earlier period than those for the anti-VEGF group (from September 2007 through September 2009).
In summary, vitrectomy combined with IVTA and macular laser photocoagulation was found to be beneficial with regard to treating non-tractional DME refractory to anti-VEGF therapy. Further controlled studies with longer follow-up durations are needed to elucidate the usefulness of triple therapy for DME in the era of anti-VEGF therapy.
Notes
No potential conflict of interest relevant to this article was reported.