Differences in the Histopathology and Matrix Metalloproteinase Expression in Tenon's Tissue of Primary Open-Angle Glaucoma and Primary Angle-Closure Glaucoma
Article information
Abstract
Purpose
To investigate the differences in the histopathology and matrix metalloproteinase (MMP) expression in the Tenon's tissue of primary open-angle glaucoma (POAG) patients, primary angle-closure glaucoma (PACG) patients, and non-glaucomatous patients.
Methods
POAG and PACG patients, who underwent a trabeculectomy and had no history of ocular disease except glaucoma, were enrolled. The number and instillation period of topical eye drops were reviewed. For the controls, which were patients without glaucoma or a history of ocular surgery, the Tenon's tissue was obtained in the course of retinal detachment surgery. For glaucoma patients, the Tenon's tissue was obtained during the trabeculectomy. H&E and Masson's trichrome staining and immunohistochemistry for MMP-1, MMP-2, and MMP-9 were performed. A total of six eyes of POAG, six eyes of PACG, and four control eyes were evaluated.
Results
The duration of topical anti-glaucoma medication and the mean number of anti-glaucoma medications were similar in the POAG and PACG groups. The levels of MMP-1 and 2 were elevated in the POAG and PACG groups compared to the control group (p=0.03, 0.01, respectively). Compared with the control group, the MMP-2 level was higher in the POAG patients (p=0.01), whereas the MMP-1 was higher in the PACG patients (p=0.04). The levels of MMP-9 in the POAG and PACG patients were not significantly different from that of the control patients (p=0.48, 0.26). The levels of MMP-2 were significantly lower in the PACG patients than in the POAG patients (p=0.02).
Conclusions
The MMP expression was altered in the Tenon's tissue of glaucoma patients compared to the control group. The levels of MMP-2 were lower in the PACG patients than in the POAG patients. These results suggest that there may be histopathological differences in the Tenon's tissue of POAG and PACG patients.
Scarring of the filtering bleb is the most common cause of failure in glaucoma filtering surgery.1,2 Wound healing is a complex process involving several phases, and the bleb failure in filtering surgery involves the proliferation of fibroblasts. Fibroblast proliferation, with the secretion of excessive extracellular matrix (ECM), is believed to play a key role in wound healing.3 Matrix metalloproteinases (MMPs)4 are a family of enzymes that are involved in tissue remodeling under various physiological and pathological conditions. Thus, the evaluation of MMP expression in glaucoma patients has implications on scarring of the filtering bleb. Moreover, the different mechanisms of primary open-angle glaucoma (POAG) and primary angle-closure glaucoma (PACG) might play a role in the variable expression of MMPs compared with normal controls.5 In a previous study, there were differences in the expression levels of MMPs between POAG and PACG as shown by the reverse transcriptase-polymerase chain reaction (RT-PCR) method.5 However, this study was not confirmed by histopathologic evaluation. The present study investigated the differences in the histopathology and matrix metalloproteinase expression in the Tenon's tissue of POAG and PACG patients and non-glaucomatous patients, who served as controls.
Materials and Methods
Patients with POAG or PACG who underwent a trabeculectomy by a single surgeon (K.H.P.) from May 2005 to January 2006 at Seoul National University Hospital were enrolled in this study. Patients with simple rhegmatogenous retinal detachment without any other ocular or systemic diseases were used as controls. The Tenon's tissue, which was obtained in the course of the trabeculectomy or surgery for retinal detachment, was obtained from an area 2-3 mm posterior to the limbus at the beginning of the operation. A sample of Tenon's tissue approximately 2×2 mm in size was excised in each case. A diagnosis of glaucoma was made based on an optic disc examination and the presence of a visual field defect. POAG was defined according to the following criteria: highest intraocular pressure (IOP) of 21 mmHg or higher without any medication, glaucomatous optic neuropathy, a glaucomatous visual field defect, an open iridocorneal angle, and no neuroradiological evidence of a non-glaucomatous cause for the optic nerve damage. PACG was diagnosed according to the following criteria: the gonioscopic verification of angle closure with an elevated IOP, the presence of peripheral anterior synechiae, and/or appositional angle closure either with acute or chronic symptoms, characteristic glaucomatous optic nerve head damage, and glaucomatous visual field loss. Patients with a prior history of ocular surgery, systemic diseases, or other ocular diseases were excluded. Informed consent was obtained from all subjects, and all performed procedures were consistent with the tenets of the Helsinki Declaration. The patients' medical records were reviewed for age, number, and instillation course of topical eye drops, and the preoperative and postoperative IOP. Six eyes from six POAG patients, six eyes from six PACG patients, and four eyes from four controls were examined.
Experimental procedures
The tissue samples from 16 patients were fixed in neutral buffered 10% formalin for 24 hours. The tissues were then embedded in paraffin wax. Four micron sections were cut and stained by routine methods with hematoxylin and eosin (H&E) for the histopathological examination and with Masson's trichrome for an evaluation of the fibrosis. Sections from the six POAG, six PACG, and four controls were examined with three antibodies according to a biotinstreptavidine peroxidase complex procedure (Dakocytomation, Carpinteria, CA, USA). The monoclonal antibodies used were anti-human MMP-1, 2, and 9 (1 in 100; Calbiochem, Cambridge, MA, USA). The dewaxed sections were subjected to antigen retrieval using 20 µg/ml proteinase kinases in 10 minute courses, and endogenous peroxidase activity was blocked by exposing the sections to 3% H2O2 for 10 minutes. The sections were incubated with the primary antibody at room temperature for 3 hours, followed by incubation with the biotinylated secondary antibody for 30 minutes at room temperature. The sections were then incubated with streptavidin conjugate for 30 minutes. Three phosphatebuffered saline (PBS) washes were performed between each incubation. After three further washes, the sections were incubated with a diaminobenzidine solution (DAB substrate, Zymed laboratory Inc., San Francisco, CA, USA), counterstained with hematoxylin for 30 seconds, and then mounted with Balssam oil. Three of the sections were prepared with PBS instead of specific antibody (ie, antibody MMP-1, 2, and 9) and used as negative controls. Specimens of a colon adenocarcinoma, which is known to express MMPs, were harvested from a patient with a colon adenocarcinoma and used as the as the positive controls.5 The cells expressing the MMPs acquired a brown-chestnut coloration in the cytoplasm, enabling their identification and quantification.
Histometric and statistical analyses
Two independent, masked observers measured the MMP expression in the subjects, using the grading scheme proposed by Shah et al.6 (Table 1). This grading was determined by comparison with the expression in the controls. The data was processed using SPSS v.12.0 software (SPSS Inc., Chicago, IL). A Mann-Whitney U test was used, and a two-sided p-value of < 0.05 was considered significant.

Results
The mean age of the POAG and PACG patients at the time of surgery was 59.0±14.6 years and 68.3±4.5 years, respectively (p=0.31). The preoperative IOP in the POAG and PACG patients was 22.2±4.4 mmHg and 27.5±17.3 mmHg, respectively (p=0.48) The mean age of the control patients at the time of surgery was 53.0±13.1 and their mean preoperative IOP was 13.5±1.3 mmHg (Table 2). The Tenon's tissues of both the POAG and the PACG patients showed significant increases in the subepithelial collagen and fibroblast density under H&E and Masson's trichrome staining. The fibrosis appeared to be more advanced in the POAG patients than in the PACG patients under H&E and Masson's trichrome staining (Fig. 1). The levels of MMP-1 and 2 were elevated in the POAG and PACG groups compared to the control group (p=0.03 and 0.01, respectively, Table 3). However, the level of MMP-9 was not significantly different between the glaucoma groups and control group (p=0.86). Comparing the POAG group and the control group, the level of MMP-2 was higher in the POAG patients (p=0.01), while the levels of MMP-1 and 9 were not different (p=0.11, and 0.48, respectively). Also, comparing the PACG group and control group, the level of MMP-1 was higher in the PACG group (p=0.04), while the levels of MMP-2 and 9 in the PACG group and the control group were not significantly different (p=0.11, and 0.26). Furthermore, comparing POAG and PACG, the level of MMP-2 was significantly lower in the PACG patients than in the POAG patients (p=0.02); however, the levels of MMP-1 and 9 were not significantly different between them (p=0.40, and 0.24).
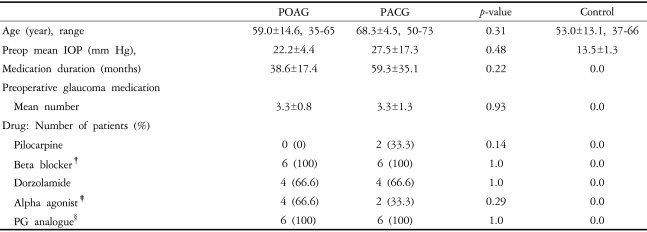
Preoperative clinical data of the glaucoma patients and control patients
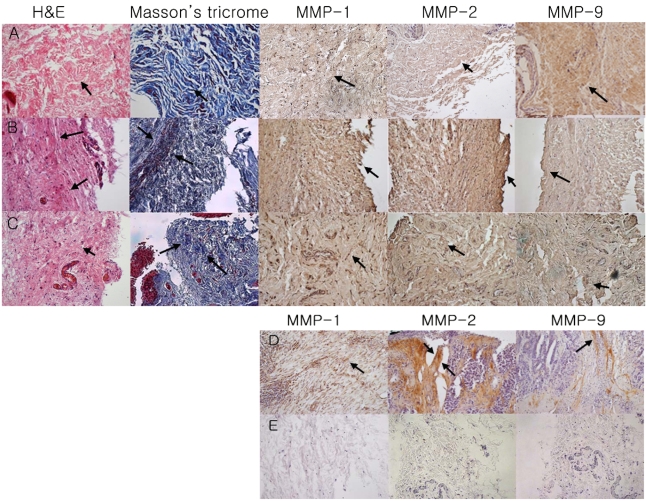
H&E stain, Masson's Trichrome stain, and immunohistochemistry of the Tenon's tissue of the control group (A), POAG group (B), PACG group (C), Positive Control (D: adenocarcinoma of colon), Negative Control (E: sections were prepared with PBS instead of primary antibody MMP-1, 2, and 9) (magnification ×200)
The Tenon's tissue of both the POAG and the PACG patients under H&E and Masson's trichrome staining showed higher subepithelial collagen and fibroblast density than that of the controls. The fibrosis under H&E and Masson's trichrome staining appeared to be more advanced in the POAG patients than in the PACG patients (arrow). Compared with the controls, the level of MMP-1 and 2 were higher in the POAG patients (grade 2, 3, respectively). The expression of MMP-2 was lower in the PACG patients than the POAG patients. The level of MMP-9 was less in POAG and PACG patients than the controls.
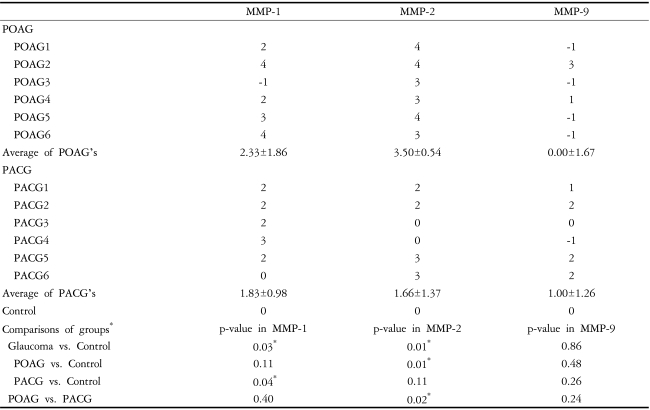
Summary of the grading of patients
Discussion
In this study, the MMP-1 and 2 expressions were increased in the Tenon's tissue samples of glaucoma groups compared to the control group, and the level of MMP-2 was lower in the PACG group than in the POAG group. MMPs are generally divided into four categories7: the collagenases, which recognize native fibrillar collagen types 1, 2, and 3; gelatinases, which degrade denatured collagens; stromelysin, which recognizes a variety of collagens; and membrane-type (MT)-MMPs, which are cell-surface bound and are involved in a variety of pericellular activities. MMPs are the major degrading enzymes of the extracellular matrix (ECM); they are involved in cell signaling, neovascularization, and activation of other proteinases.8 MMP-1 acts as a collagenase, whereas MMP-2 and 9 act as gelatinases. A previous study9 on corneal wound healing after the keratectomy showed the up-regulation of MMP-2 and 9. Liu et al.5 reported that the PACG patients had lower levels of MMP-2 mRNA in the Tenon's capsule than the POAG patients. These results agree with the results of our study, which suggest that the MMP-2 level was higher in POAG group than in the PACG group. Although, in the present study, the PACG patients had a similar IOP to that of the POAG patients, the IOP of the PACG patients was 10 mmHg higher than that of the POAG patients in Liu et al.'s study.
However, in another study,5 the PACG and POAG groups had lower MMP-2 mRNA levels in Tenon's capsule than the control group. These results were in contrast to our study results, which suggest that MMP-2 was expressed more strongly in the POAG and PACG groups than in the control group. Bradley et al.10 reported that trabecular cells might sense increases in the IOP and respond by increasing the MMP-2 and MMP-14 levels. This report provided the following clue that can explain the results of the present study: preoperative, elevated IOP can increase the expression of MMPs in both POAG and PACG patients.
MMP-9, which is known as gelatinase B, is a likely candidate for mediating the proteolysis based on its selective presence in leaking bleb tissue. Chintala et al.11 reported that MMP-9 is associated with leaking glaucoma filtering blebs and might be directly involved in the degradation of the conjunctival tissue associated with bleb failure. In this study, the levels of MMP-9 in the POAG and PACG patients were similar to those of the controls. This suggests that the leakage of a filtering bleb is not dependent on the preoperative or intraoperative conditions, but rather on the postoperative changes.
The POAG patients showed more fibrosis in the Tenon's tissue than the PACG patients (Fig. 1). This result agrees with previous studies.12-14 A histopathological image of the bulbar conjunctiva of the PACG and POAG patients receiving topical anti-glaucoma medication revealed inflammation, fibrosis, and the proliferation of fibroblasts.12 The long-term use of topical glaucoma therapy induces subclinical inflammation, and the repeated use of topical medication might induce conjunctival changes, such as squamous metaplasia, inflammation, and subconjuntival fibrosis.13 Depending on the type of medication, a significant increase in the subepithelial collagen density, degeneration of fibrocytes, and decrease in the ECM can occur. Neuciu et al.13 have suggested that these results correlate with benazalkonium chloride. This inflammatory condition activates the MMPs and degrades the ECM. Nuzzi et al.14 demonstrated that the subconjunctival connective tissue of glaucoma patients is more compact and richer in collagen fibers than that of the controls. This may be due to an effect of the medication on the subconjunctival tissue. Animal studies also have shown increased subepithelial fibrosis of the subconjunctiva in the eyes treated with topical glaucoma medication.15
In this study, even though the PACG patients underwent a similar course of topical glaucoma medication to that of the POAG patients, the POAG patients showed higher levels of fibrosis and MMP expression than the PACG patients. This suggests that factors other than the glaucoma medication are responsible for this discrepancy. The open-angle means that the anterior chamber angle structures are visible by gonioscopy.16 However, with an elevated IOP, there are many possible mechanisms17; the elements obstructing the aqueous outflow may be located on either of the following: the anterior chamber side of the trabecular meshwork, within the trabeculum, or the post-trabecular meshwork. In the post-trabecular mechanism, an obstruction of aqueous outflow can result from the increased resistance in the Schelmm's canal due to the collapse or absence of the canal or an elevated episcleral venous pressure. On the other hand, the angle-closure mechanisms include those in which the peripheral iris is in apposition to the trabecular meshwork or the peripheral cornea. The peripheral iris can be pulled or pushed into this position. The differences in mechanisms between POAG and PACG might affect the differences in uses of anti-glaucoma medications, which may result in differential expression of the ECM and MMPs.
In conclusion, the Tenon's tissue of the POAG and PACG patients showed increased fibrosis compared to the controls, and the Tenon's tissue of the POAG patients showed a higher level of fibrosis and collagen than that of the PACG patients. The levels of MMP-2 in POAG patients were higher than those in the controls. The levels of MMP-2 were lower in the PACG patients than in the POAG patients. There might be some histopathological and molecular differences in the Tenon's tissue between POAG and PACG patients. However, these results should be verified in a future study with a larger number of cases and a quantitative evaluation using the RT-PCR method proposed by Huang et al.18
Notes
This work supported by KOSEF Grant No. R01-2005-000-10875-0 and BK21.
Presented as Scientific Poster, 2006 Annual Meeting of the Association for Research in Vision and Ophthalmology, Fort Lauderdale, FL