Lens-sparing Vitrectomy for Stage 4 and Stage 5 Retinopathy of Prematurity
Article information
Abstract
Purpose
To describe the results of lens-sparing vitrectomy for the correction of retinal detachment associated with retinopathy of prematurity (ROP) and its associated complications.
Methods
Seventeen patients who underwent a lens-sparing vitrectomy for stage 4 and stage 5 ROP with plus disease at Seoul National University Children's Hospital between 1999 and 2003 were enrolled in this study. The patients who had bilateral retinal detachment of ROP underwent a lens-sparing vitrectomy in one eye and a scleral buckling surgery or lensectomy-vitrectomy in the other eye. The patients who had a retinal detachment in one eye and a regressed ROP in the other eye underwent unilateral lens-sparing vitrectomies. A review of their preoperative clinical findings (including the status of retinal detachment and plus disease), post-operative results, and any complications encountered was performed.
Results
In 17 patients, the postoperative success rate of lens-sparing vitrectomy was 58.8%. However, lens-sparing vitrectomy as a treatment for stage 5 ROP (25.0%) produced more negative post-operative results than it did when used to treat either those for stage 4a (75,0%) or 4b (66.7%) ROP. Among the 10 eyes in which the retina was attached, form vision was shown in six eyes, light could be followed by three eyes, and no light perception was present in one eye. Intra- and post-operative complications included retinal break formation, cataracts, vitreous hemorrhages, and glaucoma in patients with stages 4b and stage 5 ROP.
Conclusions
Lens-sparing vitrectomy resulted in encouraging surgical outcomes in the correction of retinal detachment of ROP, especially in stage 4 patients. Therefore, a lens-sparing vitrectomy for stage 4 ROP patient may be beneficial, although it is still associated with some intra- and post-operative complications.
Treatments for retinopathy of prematurity (ROP) include laser photocoagulation or cryotherapy (CRYO) for threshold ROP1,2 and scleral buckling surgery3-6 or vitrectomy7-12 for ROP-associated retinal detachment. The CRYO-ROP study revealed the beneficial effects of cryotherapy when used as a treatment for threshold ROP.2,13 Laser photocoagulation to the avascular retina of threshold ROP eyes proved to be just as effective (or even more effective) as cryotherapy.1 Some eyes exhibiting retinal detachment, whether they had been treated or not, required scleral buckling surgery or vitrectomy. The type of surgery depended on the extent of retinal detachment.
Scleral buckling surgery for active stage 4 ROP has beneficial effects including the relief of vitreoretinal traction and the prevention of ischemia in the detached retina, which alters the natural progression of the disease.4 However, this may not apply in stage 4 and stage 5 zone I ROP due to posterior tractional retinal detachment.14,15 Although the current standard treatment is the lens-sparing vitrectomy or lensectomy-vitrectomy, surgical outcomes in cases of stage 5 ROP are not satisfactory.16-18 The visual results achieved are low and disappointing9,12,18-21 or they present form-identification vision.10,17,22 There is still controversy concerning when surgery for stage 4 ROP should be performed and which surgical techniques have the most beneficial effects in stage 4 and stage 5 ROP.23
Lens-sparing vitrectomy in infants has been performed in the treatment of several diseases, and its main advantage is the phakic condition that results during visual rehabilitation after surgery.23-27 Lensectomy-vitrectomy produces an aphakic condition that can limit visual development during a critical period of development in infants. Scleral buckling surgery results in a myopic shift and necessitates additional surgery for buckle removal.28,29 Recently, several reports have shown that lens-sparing vitrectomy was effective in treating stage 4 ROP.30-32 Although lens-sparing vitrectomy appears to have some advantages, there is little available literature about the outcomes of this surgical technique and concerning complications from the treatment of stage 4 and stage 5 ROP. The purpose of this retrospective study is to describe the results of lens-sparing vitrectomy in the treatment of retinal detachment of stage 4 and stage 5 ROP.
Materials and Methods
Seventeen patients at Seoul National University Children's Hospital between 1999 and 2003 with stage 4 (subtotal retinal detachment) and stage 5 ROP (total retinal detachment) and with plus disease who had undergone a lens-sparing vitrectomy in at least one eye were included in this study. All patients had been treated with laser photocoagulation of the avascular retina for threshold ROP, but they had not regressed. The inclusion criterion of patients with stage 5+ ROP in the present study was a posterior total tractional retinal detachment that resulted from the progression of rush-type ROP with plus disease, i.e. the vascularized retina was limited within the zone I area.
The surgical technique for the lens-sparing vitrectomy for ROP has been described by Maguire and Trese.33 Surgery was complete when as much of the tractional membrane as possible was removed without an injury to the lens and when the entire retina was finally free from the traction. At the end of surgery an intravitreal air injection was performed for maintaining eyeball pressure, but a gas tamponade or silicone oil injection was not given. Postoperatively, spontaneous reattachment of the retina was periodically examined.
The patients with bilateral symmetric ROP disease (i.e. with the same stage and severity of plus disease in both eyes) had undergone a lens-sparing vitrectomy in one eye and a scleral buckling surgery or lensectomy-vitrectomy in the other. Both eyes underwent surgery, either simultaneously or consecutively, within several days in accordance with the systemic condition of each patient. The patients with stage 4 or stage 5 ROP with plus disease in one eye and regressed ROP in the other eye had undergone a unilateral lens-sparing vitrectomy. Data from the eyes that had undergone a lens-sparing vitrectomy only were analyzed.
Stages of ROP were defined in accordance with the international classification of ROP34 and plus disease, i.e., vascular dilation and tortuosity in the posterior pole. Patients were also subdivided into groups of both a moderate and a severe degree, in accordance with the severity of the plus disease. A moderate degree of plus disease was defined as grade 4 vascular dilation and tortuosity by Wallace et al.35 A severe degree of plus disease was characterized by more severe vascular dilation and tortuosity than was seen in grade 4. Informed consent was obtained from the parents of all participants before sedation for examination and surgery.
A review of the pre-operative clinical findings, post-operative results, and any complications was performed, and the results of the lens-sparing vitrectomy were compared in accordance with the stages. Anatomical success was defined as an attachment of the retina, at least in the posterior pole, during the post-operative follow-up periods. For the evaluation of visual development at the last follow-up, vision was classified into three categories: form vision (patients can fix their eyes on a small moving toy), light follow (patients can fix their eyes on a moving pen-light), and light perception (patients can differentiate between the light on and off).
Results
Seventeen patients comprised the study population, and ten of the patients were females. The mean gestational period was 28.8 weeks (range: 25-34 weeks) and the mean birth weight was 1224 grams (range: 800-1870 grams). The mean post-operative follow-up period was 2.2 years (range: 1.1-4.8 years).
The eight bilateral symmetric patients underwent a lens-sparing vitrectomy in one eye. Among them, three patients had scleral buckling surgery while the other five had the lensectomy-vitrectomy in the other eye. The nine unilateral patients underwent a lens-sparing vitrectomy in only one eye. Their other eyes had regressed without retinal detachment, which was resultant from the laser photocoagulation. Pre-operative stages of ROP and post-operative results are summarized in Table 1.
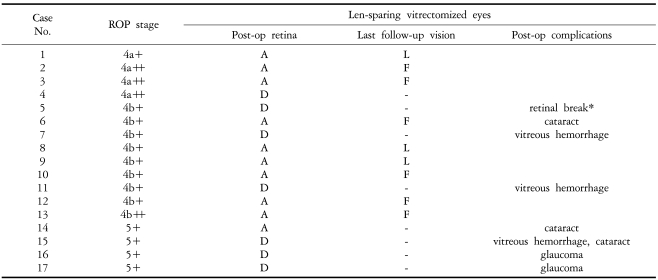
Surgical outcome of lens-sparing vitrectomized eyes for stage 4 and stage 5 retinopathy of prematurity
At the last follow-up examination, visual development was assessed in ten eyes in which the retina was post-operatively attached. Form vision was seen in six of these eyes, light follow was noted in three eyes, and no light perception was found in one. None of the eyes in which the retina was not attached had light perception.
Among the 17 cases of lens-sparing vitrectomy, cataracts and dense vitreous hemorrhages occurred as a post-operative complication in three patients. Two of these patients required lens surgery due to dense cataracts, and the remaining one patient did not require surgery but experienced mild lens opacity. Three occurrences of dense vitreous hemorrhage were observed, and they all resulted in a failure of the retina to reattach. In one of the unilateral patients, a retinal break was noticed during surgery which caused a failure of retinal reattachment. Two patients with stage 5 ROP experienced the post-operative complication of angle-closure glaucoma.
The overall anatomical success rate was 58.8% (10/17), and the post-operative results of stage 4 ROP patients were better than those with stage 5 ROP (Table 2).
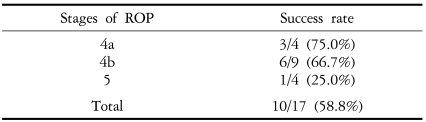
Overall success rate of lens-sparing vitrectomy for stage 4 and stage 5 retinopathy of prematurity
Discussion
Lens-sparing vitrectomy in infants has been used to treat tractional retinal detachment and vitreous hemorrhage associated with ROP, non-clearing preretinal hemorrhage secondary to shaken-baby syndrome, and posterior persistent fetal vasculature.23-26,30-33 Although this procedure tends to be more difficult in infants than in adults or children because of their relatively large lens size compared to the posterior segment of their eye, it can cautiously be done without damage to the lens. The crystalline lens in infants can be spared by employing a two-port pars plicata approach, and also by inserting instruments parallel to the visual axis.35 After lens-sparing vitrectomy in infants, 67% of the lenses remained clear after an average follow-up time of 27 months.25 Our results showed that three cases of cataract formation had occurred after an average follow-up time of 2.2 years, and that 82.4% of the lenses remained clear after surgery. Only two of these required further surgery.
Recently, Hartnett23 reported that a poor surgical outcome after surgery for stages 4 and 5 ROP was related to the presence of vitreous organization, neovascularization, and plus disease. Surgical procedures included scleral buckling, lensectomy-vitrectomy, and lens-sparing vitrectomy, but similar outcomes resulted from scleral buckling and lens-sparing vitrectomy in those with stage 4b ROP. Capone and Trese26 reported that 90 percent of the eyes with stage 4a ROP exhibited successful retinal reattachment after lens-sparing vitrectomy. Our results also showed a success rate of 75% and 66% for stages 4a and 4b each. The success rate plummeted to 25% for stage 5 patients. In the present study, lens-sparing vitrectomy produced better results in cases of stage 4 ROP than in patients with stage 5.
Hartnett23 found that the surgical outcome was not associated with the type of surgery chosen for stage 4 ROP, so it was of no consequence if the surgery used was scleral buckling surgery or lens-sparing vitrectomy. She also insisted that lensectomy-vitrectomy should be reserved only for stage 5 eyes with narrow funnel-type detachments, and that it was necessary to attempt a lens-sparing vitrectomy intervention before a tight funnel-type total retinal detachment could develop. Our data supported this, and also suggested some utility of the lens-sparing vitrectomy in stage 5 ROP patients with plus disease. However, in cases of open funnel-type retinal detachments, the lens-sparing vitrectomy resulted in rather disappointing outcomes, and it was associated with significant postoperative complications. Among the four patients who underwent lens-sparing vitrectomy for stage 5 ROP with plus disease, two later showed pupillary block glaucomas and one manifested a vitreous hemorrhage and a cataract. Therefore, in these cases, lens-sparing vitrectomy should be avoided. In addition, Maguire and Trese24 reported that cataracts developed in two out of three eyes with stage 5 ROP after lens-sparing vitrectomy.
The presence of plus disease in stage 4 and stage 5 ROP is also a predictor of poor surgical outcome.23 There is a wide range in the severity of the disease,31 so we created a division between moderate cases and those of a more severe degree. The severity of plus disease may not influence the surgical outcome, but its presence may be rather important by itself. All cases in this study exhibited progressive retinal detachment with plus disease in spite of previous treatment with laser photocoagulation. This is, in part, a cause of the failure of retinal reattachment and intra- or post-operative vitreous hemorrhage. If our study patients had had a lower incidence of plus disease, our surgical outcomes would have very likely been better. Glaucoma and vitreous hemorrhage were both reported to be causes of poor outcomes in severe ROP.19,36 Our results also revealed retinal reattachment failure after lens-sparing vitrectomy in cases that also had such complications. To avoid this, lens-sparing vitrectomy should be performed before stage 5 ROP develops, and also in the absence of plus disease. If the plus disease presents as a severe condition, there will be a higher probability of intra-operative and post-operative complications, and the surgical prognoses should be guarded.
Luna et al.37 reported that peripheral retinal laser photocoagulation before lens-sparing vitrectomy for stage 4a ROP eyes affected surgical outcomes. Without laser photoablation before surgery, the organized vitreous was easier to cut and the retina was less rigid and could be smoothly flattened. Conversely, with pre-surgical laser photoablation, the organized vitreous became more difficult to manipulate, and the retina became more rigid. All the members of our study had undergone laser photocoagulation before surgery, so our study cannot speculate on the differences observed by the previous study. The observation by Luna et al. may or may not be true, but the difficulty of surgical manipulation and the retinal rigidity seem to depend more on the fibrovascular proliferative changes of the detached retina than on any pre-operative procedure.
In the treatment of stage 5 ROP, the lens-sparing vitrectomy produced less-than-desirable results, but in the treatment of stage 4a or stage 4b ROP, the lens-sparing vitrectomy yielded rather promising results. However, several limitations of this study should be noted. One is the small case number of our study. The second limitation is that we could not standardize the gestational age and birth weights of our subjects. Further studies with a larger number of patients are required in order to determine the timing and criteria for surgery to treat stage 4 ROP, and also to decide which surgical technique is the most desirable for treatment of stage 4 and stage 5 ROP.
In summary, we described the results of lens-sparing vitrectomy as a treatment for stage 4 and stage 5 ROP. Surgical outcomes for stage 4 ROP produced better post-operative results than those for stage 5. Some cases manifested such post-operative complications as cataracts, vitreous hemorrhages, glaucoma, and the formation of retinal breaks. These results demonstrate that while lens-sparing vitrectomy may be beneficial in cases of stage 4 ROP, it is certainly not without risk of complications.