Peters Anomaly in One Premature Twin Following Hydroxychloroquine Exposure During Pregnancy: A Case Report
Article information
Dear Editor,
Peters anomaly is the most common cause of congenital corneal opacity. It commonly presents bilaterally and sporadically, but it is sometimes inherited in the autosomal dominant or recessive patterns [1]. Its cardinal feature is central corneal opacity and iris strands adhered to the posterior cornea, with defects that can occur throughout the whole layers in the cornea from the endothelium to stroma [2]. Previous reports suggest that Peters anomaly is related to prematurity, fetal alcohol syndrome, intrauterine infections, and antenatal teratogenic exposure [3]. Herein, we report a case of Peters’ anomaly in one premature twin with antenatal hydroxychloroquine exposure. Written informed consent for publication of the research details and clinical images was obtained from the patient’s mother. To the best of our knowledge, this is the first report of a Peters anomaly case following hydroxychloroquine exposure during pregnancy in Korea.
A 2-day-old female infant was referred by the pediatric department for presenting a visible corneal opacity in her left eye. She is one of the twins born first at 34 gestational weeks, weighing 2.06 kg, via Cesarean section due to preterm labor. The second twin showed no anomaly in eye globes and no systemic findings. Her former brother who was born at 33 gestational weeks weighing 1.5 kg died at 2 years of age due to pulmonary hypertension. Her mother tested positive for antinuclear antibody, thyroglobulin antibody, and antithyroid microsomal antibody. Therefore, she had been treated with aspirin 100 mg/day and hydroxychloroquine 300 mg/day to manage the rheumatoid disease. The hydroxychloroquine treatment was continued throughout the pregnancy.
During the eye examination, central corneal opacities which were more prominent in the left eye were noted with iris-cornea strands and lens-cornea strands in both eyes (Fig. 1A–1D). The intraocular pressures were 15 mmHg in both eyes. No definite signs of lens opacity or retinopathy of prematurity were seen in both eyes. Systemically, patent foramen ovale and intraventricular hemorrhage were noted.
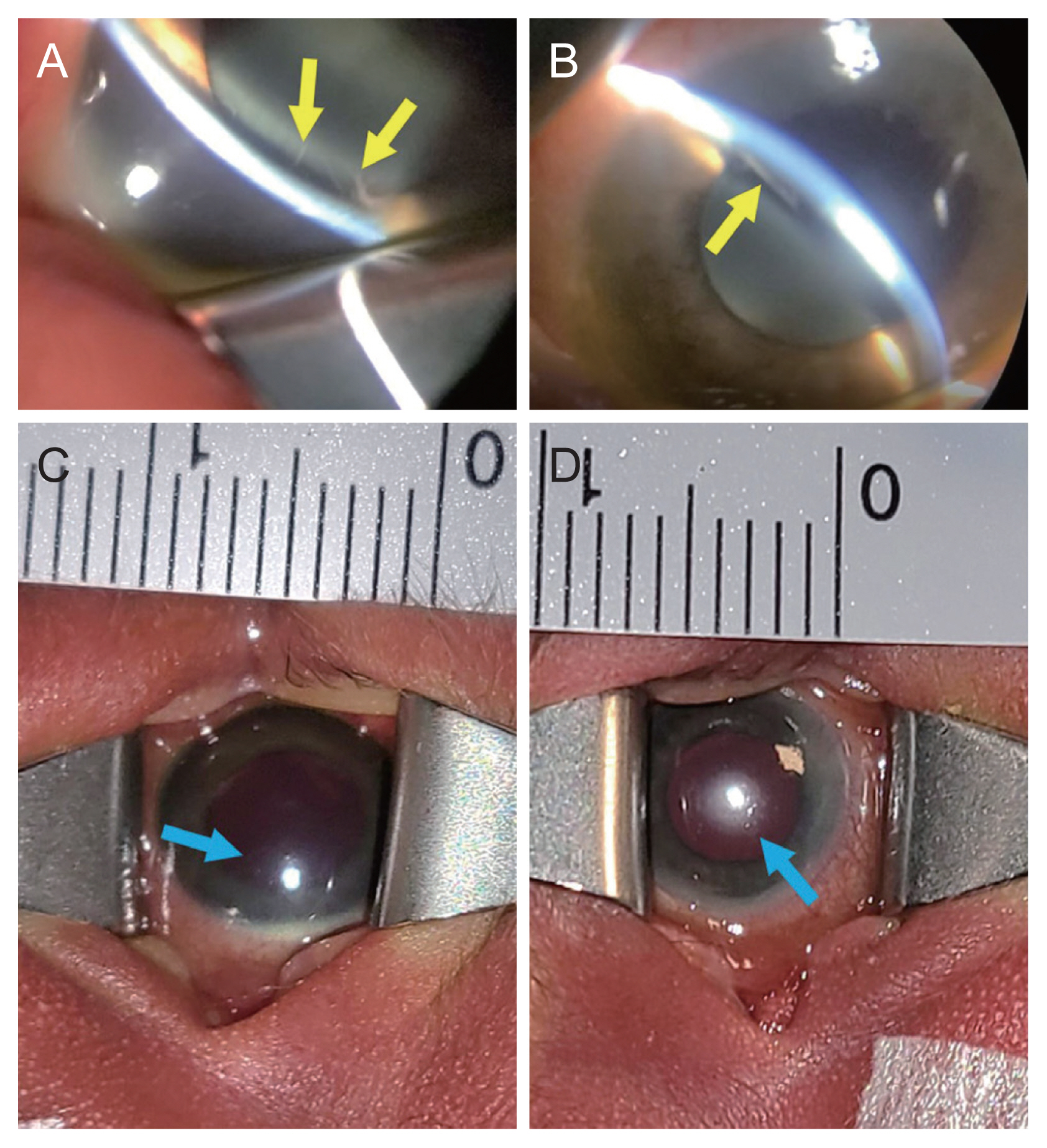
Anterior segment photography of patient with Peters anomaly. Slit-lamp images of (A) the right eye and (B) left eye demonstrating iris-lens adhesions and cornea-lens strands (yellow arrows). Photographs of (C) the right eye and (D) left eye showing central round corneal opacity (blue arrows). Note that the corneal opacity of the right eye is located more nasal compared to that of the left eye.
This Peters anomaly case is intriguing because the previous report of its occurrence and the antenatal exposure history to hydroxychloroquine is rare. Costedoat-chalumeau et al. [4] reported that no ocular abnormalities were seen in the children of 133 mothers with rheumatoid disease treated with hydroxychloroquine during pregnancy. Another teratogen associated with anterior segmental dysplasia, 2-Chloro-2′-deoxyadenosine, is known to induce microphthalmia and keratolenticular dysgenesis in mice. Additionally, there have been reports of Peters anomaly due to fetal alcohol exposure. By far, there is only one case report which describes the possible relationship between Peters anomaly and hydroxychloroquine treatment, although the case was superimposed with the concomitant exposure to methotrexate as well. Hydroxychloroquine is an antimalarial agent and there is no evidence so far that its use during pregnancy is harmful [5]. However, it is a lipophilic weak base so it can easily pass through the plasma membranes and transfer into breast milk [4]. Therefore, the addition of our report to existing literature indicates the possible link between bilateral Peters’ anomaly and maternal exposure to hydroxychloroquine.
Acknowledgements
None.
Notes
Conflicts of Interest: None.
Funding: None.