Successful Femtosecond Laser-assisted Cataract Surgery for a Cataract with Persistent Pupillary Membrane: A Case Report
Article information
Dear Editor,
The persistent pupillary membrane (PPM) is a remnant of the tunica vasculosa lentis, which provides blood supply for fetal crystalline lens development. During normal fetal development, the tunica vasculosa lentis undergoes involution and disappears between the 8th and 9th gestational months. The PPM develops due to incomplete atrophy of the fetal pupillary membrane [1]. Rarely, if a thick PPM covers the visual axis, administration of topical atropine or surgical intervention is required to prevent the progression of amblyopia and improve visual acuity [1]. Previous studies have reported on the surgical excision of a remnant membrane with cataract surgery or neodymium-doped yttrium aluminum garnet (Nd-YAG) laser lysis of the PPM before phacoemulsification [2,3].
Femtosecond laser-assisted cataract surgery (FLACS), which includes three main steps (corneal arcuate incision, anterior capsulotomy, and lens fragmentation), is an advanced technology that increases the accuracy and reduces the complications compared to conventional cataract surgery [4]. The advantages of FLACS include astigmatism correction, increased stability of the implanted intraocular lens with reproducibility and accuracy of capsulotomy, and reduced use of ultrasound [4]. Capsulotomy performed using the femtosecond laser can excise the PPM, reduce the risk of intraoperative bleeding, and help ensure visibility of the surgical field [5].
Here, we report a case in which a cataract in an eye with a PPM was treated by FLACS. Written informed consent for publication of this case and clinical images was obtained from the patient.
A 61-year-old female patient presented to the ophthalmology department of Severance Hospital with bilateral decreased visual acuity and visual discomfort. She had diabetes mellitus but had no history of ocular trauma or operation and no familial ocular disease. Her preoperative corrected distant visual acuity (CDVA) was 0.3 (decimal) with autorefraction −3.00 diopters (D) −1.50 D × 138° in the right eye and 0.7 (decimal) with +2.25 D −0.75 D × 84° in the left eye. The intraocular pressure was 17 and 18mmHg in the right and left eyes, respectively, using a noncontact tonometer. On slit-lamp examination, we observed cataracts with nuclear opacity grade 3 by Lens Opacities Classification System III classification in her both eyes and PPM in her right eye. The pupillary threads were superotemporally connected to the other parts of the iris and attached to the anterior lens capsule (Fig. 1A). Although the PPM did not completely cover the pupil, it was suspected to adversely affect her visual acuity with the cataract in the right eye. The patient was scheduled to undergo FLACS in both eyes, with an interval of 1 week between the left and right eye.
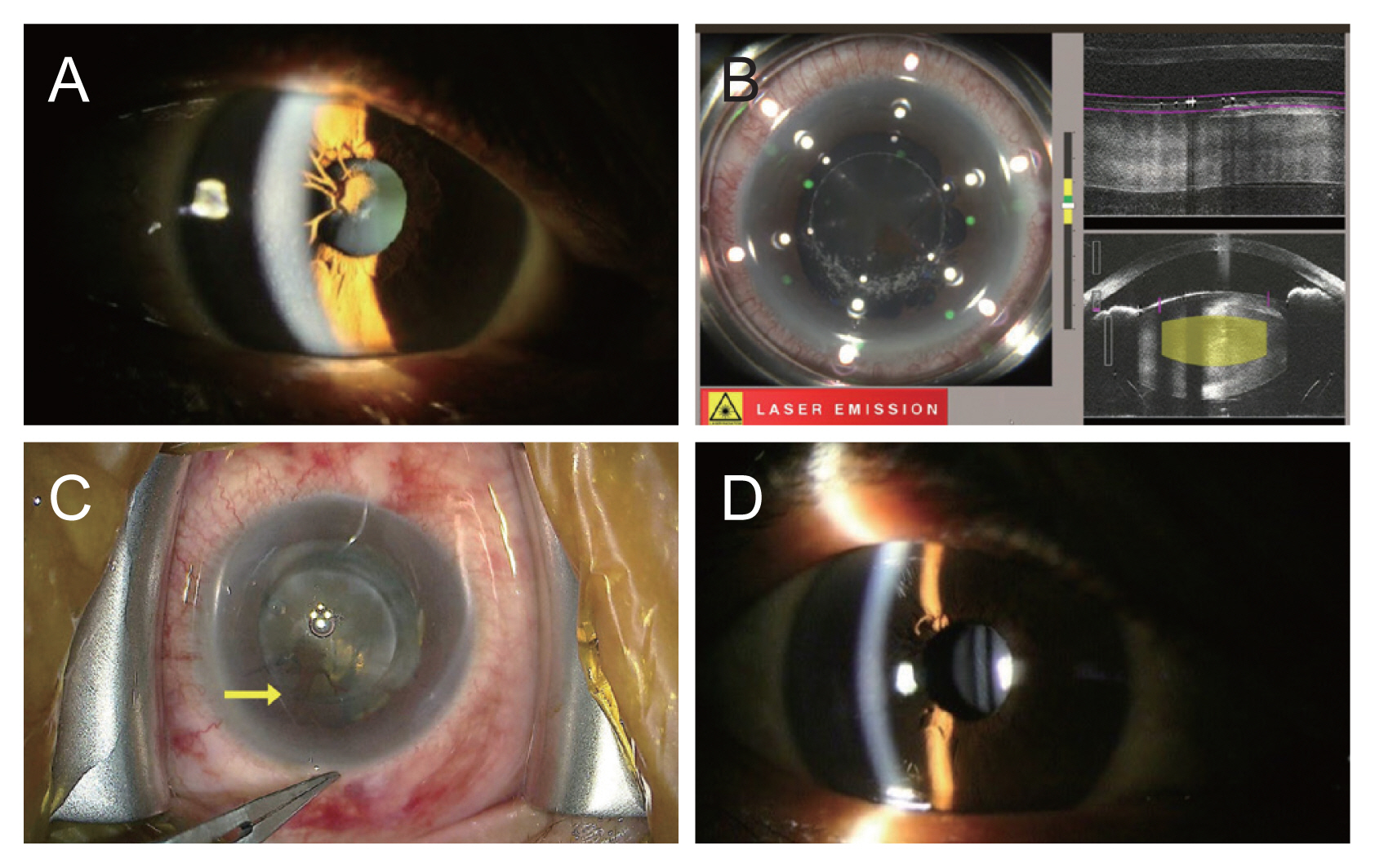
Preoperative, intraoperative, and postoperative images. (A) Persistent pupillary membrane (PPM) attached to the lens with cataract in a 61-year-old female patient (preoperative slit-lamp photograph). (B) Capsulotomy step of femtosecond laser excising the PPM. (C) PPM excised following femtosecond laser (arrow). (D) The right eye with the perfectly round pupil after femtosecond laser-assisted cataract surgery (slit-lamp photograph at 1-week postoperative follow-up).
We used a LenSx femtosecond laser system (Alcon, Aliso Viejo, CA, USA). Most of the PPM strands were disconnected during the anterior capsulotomy step using the femtosecond laser (Fig. 1B, 1C). However, anterior capsulotomy was suspected to be incomplete on the side of the thick strands. The capsulotomy was completed by holding the edge of the anterior capsule using capsulorhexis forceps and pulling it carefully toward the center of the lens. The cut PPM and anterior capsule were successfully removed together, and the remaining surgical procedures were completed without any problems.
The postoperative follow-up showed a perfectly round pupil with removed PPM and an adequately positioned intraocular lens in the bag (Fig. 1D). The patient revealed a stable course without complications like intraocular pressure elevation, infection, and macular edema. At the 1-month postoperative follow-up, her CDVA was 1.0 (decimal) in both eyes with manifest refraction −0.25 D × 90° in the right eye and −0.50 D in the left eye, respectively.
This case shows that PPM can be removed concurrently with cataract surgery using a femtosecond laser, without additional procedures for PPM. FLACS may be easier to make a round pupil and reduce the possibility of intraoperative complications such as hyphema than direct surgical resection [3,5]. Compared to usual cataract cases without PPM, the risks of iris bleeding and anterior capsular tear following incomplete capsulotomy may increase. Therefore, the operator needs to adjust the position of capsulotomy in the femtosecond laser to cut the relatively thin point of PPM, and the capsulotomy must be finished manually, ensuring that it has been performed completely after the femtosecond laser.
In conclusion, FLACS can be a useful treatment option for cataracts with PPM, although removal of PPM and anterior capsulotomy must be performed carefully following femtosecond laser application.
Acknowledgements
None.
Notes
Conflicts of Interest: None.
Funding: None.