Accuracy of the Hand-held Wavefront Aberrometer in Measurement of Refractive Error
Article information
Abstract
Purpose
To compare refractive error measured by hand-held wavefront aberrometers with postcycloplegic autorefraction (AR) and cycloplegic refraction (CR).
Methods
The medical records of patients who received refractive measurements using the wavefront aberrometer, postcycloplegic AR, and CR between January 2014 and January 2016 were retrospectively analyzed. The mean differences, 95% confidence intervals, and limits of agreement (LOA) were calculated for the refractive vector components (M, J0, and J45).
Results
Fifty-one patients (9.0 ± 5.5 years, male 41.2%) were enrolled in this study, and only the right eye of each was included. Refractive errors ranged from −9.25 to +7.25 diopters (D) for spherical equivalent (median, 0.75 D). The M component was not significantly different among the three methods (p = 0.080). However, the J0 vector component was significantly different (p < 0.001). After post hoc analysis, the wavefront aberrometer obtained more positive values for J0 compared to the other methods. The J45 component was not significantly different among the three methods (p = 0.143). The mean difference between the wavefront aberrometer and postcycloplegic AR was −0.115 D (LOA, −1.578 to 1.348 D) for M, 0.239 D (LOA, −0.371 to 0.850 D) for J0, and −0.015 D (LOA, −0.768 to 0.738 D) for J45. The mean difference between the wavefront aberrometer and CR was −0.220 D (LOA, −1.790 to 1.350 D) for M, 0.300 D (LOA, −0.526 to 1.127 D) for J0, and −0.079 D (−0.662 to 0.504 D) for J45.
Conclusions
The wavefront aberrometer showed good agreement with postcycloplegic AR and CR in spherical equivalents, but tended to produce slightly myopic results. The wavefront aberrometer also overestimated with-the-rule astigmatism. Therefore, we recommend that the device be used for estimations of refractive error, which may be useful for patients who have postural difficulties, live in undeveloped countries, or are bedridden.
Uncorrected refractive errors are a major cause of amblyopia, which interrupts social functioning and academic performance in children [1]. It is estimated that over one billion people suffer from uncorrected refractive errors worldwide [23]. The incidence rate of amblyopia caused by uncorrected refractive errors is generally higher in low-income or under-developed countries [45]. With proper diagnosis and early management of refractive errors in children, amblyopia can be treated quickly, which can greatly contribute to improving quality of life. Previous studies have shown that eye screening and correcting refractive errors has the potential to improve social and academic functioning, especially in low-income patients [67].
Refractive errors can be measured in several ways, including (1) Objective refraction using an auto kerato-refractometer (autorefraction, AR), (2) cycloplegic refraction (CR) using retinoscopy, or (3) with a wavefront guided aberrometer. CR is the gold standard for measuring refractive errors, and is still commonly used. However, these procedures have some weaknesses. First, they take a long time and require properly trained optometrists or ophthalmologists. They also show poor test-retest reliability and are easily affected by the technician's ability [89]. AR is commonly used as a starting point for subjective refraction and is mostly used in settings with high resource availability. In comparison to the other techniques, AR does not require experienced operators, and is faster and easier to perform [101112]. A wavefront aberrometer is an instrument used to detect the incompleteness of the human optic system at the level below the wavelength of light. Wavefront aberrometer measurements can be categorized according to numerous principles, including Hartmann-Shack, Tscherning, laser ray tracing, and slit sciascopy [13]. Hartmann-Shack sensors are used in ophthalmology to identify visual deficits prior to corneal treatment for complex refractive disorders [814]. Unlike objective refraction, subjective manifest refraction attempts to determine refractive errors by trial and error with the patient's cooperation. Through patient interaction, manifest refraction allows clinicians to provide more comfortable eyeglasses for patients. However, it is more time consuming and requires more clinical experience to perform than objective refraction. Additionally, manifest refraction can be inaccurate in patients (especially children) with high accommodative reserve. Therefore, a cycloplegic agent is necessary to relax the accommodative reserve due to the accommodative blur drive which produces myopic over-correction [151617].
The OVITZ P10 (Ovitz Corporation, Rochester, NY, USA) is a hand-held device used for measuring refractive error using the aberrations of the eye with a Hartmann-Shack wavefront sensor. After acquiring images from wavefront sensing, it uses Zernike decomposition to filter low-order refractive errors from high-frequency aberrations [18]. The device converts Zernike defocus and astigmatism terms into the conventional sphere, cylinder, and axis format. Typically, the device is used for measurement in patients in under-developed countries, or who are bed-ridden or in a wheelchair and may have difficulty with a table-mounted autorefractor (Fig. 1). The aim of this study is to investigate the accuracy of refractive error measurement using a wavefront aberrometer by comparing results to those obtained by postcycloplegic AR and CR.
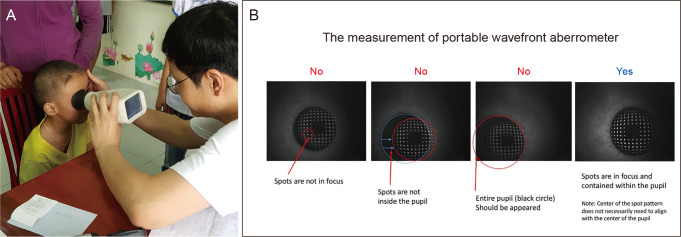
The measurement of portable wavefront aberrometer. (A) Measurement with the portable OVITZ P10 wavefront aberrometer. (B) Once the device had been positioned properly, the examiner was able to see the array of Hartmann-Shack images on the screen. The array of Hartmann-Shack spots should be clearly focused, and contained within the pupil.
Materials and Methods
The study was conducted at the Severance Hospital, Yonsei University College of Medicine, Seoul, South Korea and was approved by the institutional review board (4-2019-0743). The study also adhered to the tenets of the Declaration of Helsinki. Written informed consent was waived due to the retrospective nature of the study. The medical records of patients who underwent refractive measurement using a wavefront aberrometer, AR, and CR between January 2014 and January 2016 were retrospectively reviewed. Before starting measurements, patient history, visual acuity, tonometry, slit-lamp examination, fundus examination, and tonometry with a non-contact tonometer were obtained. Patients who had strabismus or refractive errors were included in the study. Patients who had previous corneal or retinal surgery were excluded. Patients who had anterior or posterior segment pathology, including retinopathy or prematurity, were excluded. A total of 51 eyes from 51 patients were analyzed in this study.
Cycloplegia was achieved with three consecutive instillations of 1% cyclopentolate hydrochloride (OcuCyclo; Samil, Seoul, Korea) and 0.5% tropicamide with 0.5% phenylephrine (Mydrin-P; Santen Pharmaceutical, Osaka, Japan), administered 5 minutes apart. The measurement of refractive errors was performed 1 hour after the instillation of the first drop. Adequate cycloplegia was defined as having a subjective amplitude of accommodation less than 2 diopters (D). This was assessed by measuring the push-up amplitude of accommodation with a supplementary +2.00 D lens added to the distance refractive correction. Subsequently, the refractive error of the subject's eye was assessed in the following order: (1) postcycloplegic AR, (2) CR using retinoscopy, and (3) a hand-held wavefront aberrometer.
Postcycloplegic AR was measured with a table-top auto refractometer (KR-1; Topcon, Tokyo, Japan). First, the patient was seated in front of the on-table auto refractometer, and instructed to place their chin on the chin rest. The physician then ensured that their forehead was touching the forehead rest. After instructing the patient to watch the object on the monitor, the measurement was taken. CR was performed by a single pediatric ophthalmologist for all cases. A trial lens set with retinoscopy was used for CR. The OVITZ P10 wavefront aberrometer was used to obtain five successive readings after cycloplegia, and the values were averaged. When recording refractive error with the OVITZ P10, alignment was achieved by having the subject look into the instrument. The unexamined eye was covered by the patient's hand (Fig. 1A). The patient could see a bright red spot. Once the device had been positioned properly, the examiner was able to see the array of Hartmann-Shack images on the screen (Fig. 1B). When performing measurements, we tried to minimize head or instrument tilting as much as possible. To obtain AR data, the internal software reduced the evaluated pupil size to a diameter of 3 mm.
Refractive error values were obtained from the devices with the conventional notation of sphere (S), minus cylinder form (C), and cylindrical axis (α). All results were converted into power vectors (M, J0, and J45), as described by Liu et al. [19]; spherical equivalent (SE) refraction as M = S + C/2, “with-the-rule” and “against-the-rule” astigmatism (Cartesian astigmatism) as J0 = (−C/2)cos(2α), and oblique astigmatism as J45 = (−C/2)sin(2α). In our study, the mean SEs between the right and left eyes were highly correlated (Spearman correlation coefficient = 0.955, p < 0.001), therefore, only the measurement from the right eye of each patient was analyzed.
Assuming an effect size of 0.25, type I error of 0.05, 90% power, and a non-sphericity correction e 0.8, the required sample size was 42 subjects using G power 3.1.9.5 (Heinrich-Heine-Universitat, Dusseldorf, Germany) [20]. Statistical analyses were performed using STATA ver. 13.1 (StataCorp., College Station, TX, USA). A p-value less than 0.05 was considered statistically significant. Repeated measures analysis of variance (ANOVA) and post hoc analysis using the Tukey test were performed for statistical comparison.
Results
Among 51 patients, the mean age was 9.0 ± 5.5 years, and 21 patients (41.2%) were male. The patients had a wide range of refractive errors, ranging from −9.5 to +7.25 D SE (median, 0.75 D), and the mean astigmatism was −0.69 D (median, −0.5; range, −3 to 0 D). In addition, 21 patients (31.0%) had an astigmatism value of at least −1.00 D. The mean values and standard errors of M, J0, and J45 for the three measurement methods, shown in Table 1, were compared using repeated measures ANOVA. The M value was not significantly different among the three methods (p = 0.080, repeated measures ANOVA). The M obtained from the wavefront aberrometer (0.05 ± 3.77 D) was slightly more myopic than that of CR (0.27 ± 3.34 D, p = 0.064, post hoc Tukey test). The J0 value was significantly different between the three methods (p < 0.001). With post hoc analysis, J0 between postcycloplegic AR and wavefront aberrometer was significantly significant (mean J0, 0.37 vs. 0.61; p < 0.001), and J0 between CR and wavefront aberrometer was also significantly different (mean J0, 0.31 vs. 0.61; p < 0.001). There was no significant difference in J0 between postcycloplegic AR and CR (p = 0.517). The J45 component was not significantly different among the three methods (p = 0.143). With post hoc Tukey analysis, the J45 components were not significantly different (postcycloplegic AR vs. CR, p = 0.289; CR vs. wavefront aberrometer, p = 0.151; postcycloplegic AR vs. wavefront aberrometer, p = 0.931).

Mean values of power vectors measured by three different measurement techniques
In subgroup analysis of astigmatism, vector components in patients who had cylinder values of 0.75 D or larger (n = 26) with AR, the J0 value was significantly different between the three methods (p = 0.001). With post hoc analysis, J0 between postcycloplegic AR and wavefront aberrometer was significantly different (mean J0, 0.70 vs. 0.95; p = 0.047), and J0 between CR and wavefront aberrometer was also significantly different (mean J0, 0.54 vs. 0.95; p < 0.001). There was no significant difference in J0 between postcycloplegic AR and CR (p = 0.229). The J45 component was not significantly different among the three methods (p = 0.225). The mean difference of M between the wavefront aberrometer and postcycloplegic AR was −0.115 D.
To compare the differences between AR, CR, and the wavefront aberrometer, the 95% limits of agreement (LOA) were quantified using the technique described by Bland and Altman [21]. The difference between each vector measurement with respect to the wavefront aberrometer was determined, and the LOA was calculated as 1.96 multiplied by the standard deviation of the differences [21]. Between the wavefront aberrometer and postcycloplegic AR, the mean M difference was −0.115 D, and the LOA for M was −1.578 to 1.348. For J0, the mean difference was 0.239 D, and the LOA was −0.371 to 0.850. For J45, the mean difference was −0.015 D, and the LOA was −0.768 to 0.738. Between the wavefront and CR, the mean M difference was −0.220 D, and the LOA was −1.790 to 1.350. The mean difference was 0.300 D and the LOA was −0.526 to 1.127 for J0. The mean difference for J45 was −0.079 D and the LOA was −0.662 to 0.504 (Fig. 2A–2F).
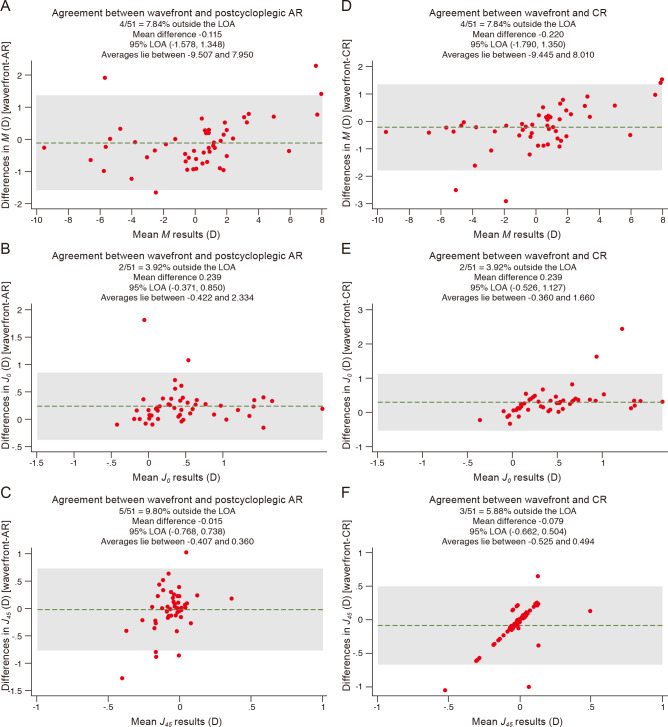
Bland-Altman plot showing the differences between wavefront aberrometer and postcycloplegic autorefraction (AR) (left), wavefront aberrometer and cycloplegic refraction (CR) (right) in 51 patients at each power vectors (M, J0, J45). Agreement between the wavefront aberrometer and postcycloplegic AR, (A) the mean M difference was −0.115 diopters (D), and the limits of agreement (LOA) was −1.578 to 1.348. (B) For J0, the mean difference was 0.239 D, and the LOA was −0.371 to 0.850. (C) For J45, the mean difference was −0.015 D, and the LOA was −0.768 to 0.738. Between the wavefront and CR, (D) the mean M difference was −0.220 D, and the LOA was −1.790 to 1.350. (E) The mean difference was 0.300 D and the LOA was −0.526 to 1.127 for J0. (F) The mean difference for J45 was −0.079 D and the LOA was −0.662 to 0.504.
The axes of the cylindrical components measured using the wavefront aberrometer were compared to AR and CR in patients with cylinder 0.75 D or more (n = 26). Compared to AR, only 46.2% of the cylinders were within 5.0°; 61.5% were within 10°, and 76.9% were within 20°. Compared to CR, 61.5% were within 5.0°, 76.9% were within 10°, and 96.2% were within 20° (Table 2).
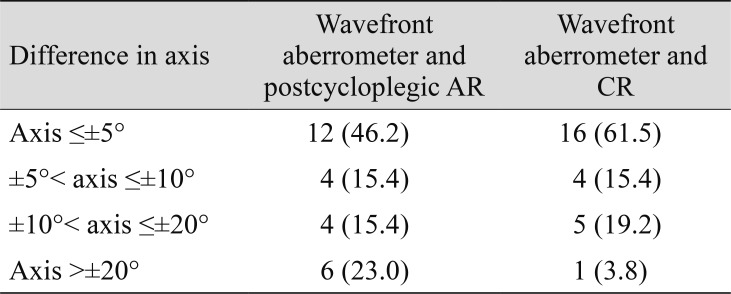
Comparison of axes of the cylindrical components between wavefront aberrometer, postcycloplegic AR, and CR in subjects with cylinder 0.75 diopters or more with AR (n = 26)
Discussion
In this study, we investigated the accuracy of a handheld wavefront aberrometer for measuring refractive errors compared to conventional methods including AR and CR. Our results indicate that the M values were not significantly different among the three methods. The wavefront aberrometer showed a slight myopic shift compared to the other methods, but the difference was not statistically significant. J0 refers to cylinder power set at orthogonally 90° and 180° meridians, representing Cartesian astigmatism [19]. The vector values in J0 tended to be more positive in measurements made with the wavefront aberrometer (p < 0.001), indicating the trend toward with-the-rule astigmatism. This trend was also observed in patients who had cylinder 0.75 D or more. J45 refers to a cross-cylinder set at 45° and 135°, representing oblique astigmatism. The oblique astigmatism component was not significantly different among the three methods. Because our subjects were children, they usually had with-the-rule astigmatism. As the wavefront aberrometer showed slight myopic shift in SE, the astigmatism component presented by minus cylinder is also expected to be overestimated.
Previous studies compared refractive error measurements between hand-held or table mounted AR, wavefront aberrometers, and CR. Liang et al. [22] compared handheld and table mounted AR in both cycloplegic and non-cycloplegic conditions. With hand-held AR, the mean myopic bias was 0.59 D under non-cycloplegic conditions. However, there were no significant differences between hand-held and table-mounted AR under cycloplegic conditions. Iuorno at el. [23] compared hand-held AR under non-cycloplegic conditions to CR with retinoscopy in 91 children. They reported that hand-held AR results were more myopic than CR. Although all refractive measurements were taken after cycloplegia, some residual accommodation might have remained. The other eye was occluded during wavefront aberrometer measurement, and the subject was required to look into the instrument. Therefore, this might explain the slight myopic shift in SE with the wavefront aberrometer.
Previous studies also compared wavefront aberrometers with AR and subjective refraction. Early wavefront aberrometers, such as the complete ophthalmic analysis system, were reported to have similar accuracy to AR [242526]. Pesudovs et al. [27] compared the complete ophthalmic analysis system aberrometer with AR and subjective refraction, and found significant levels of similarity between the three devices. Bennett et al. [28] compared the wavefront aberrometer based on dynamic sciascopy to AR and subjective refraction. AR and the wavefront aberrometer showed agreement with subjective refraction. Although AR showed slightly higher levels of agreement than the wavefront aberrometer in their study, the difference was not significant. The table-mounted wavefront aberrometer has also been compared with CR. Fernandez de Castro et al. [29] compared CR with three different wavefront aberrometers based on the Hartmann-Shack principle in 55 subjects. Although there were small differences between the three devices, all of the devices correlated well with CR in this study.
In our study, the hand-held wavefront aberrometer showed good agreement with low bias in M (−0.115 D with AR, −0.220 D with CR). Unlike M, the cylinder measurements were significantly different. The bias was −0.239 D with AR and 0.300 D with CR in the J0 component, showing significant differences in Cartesian astigmatism. In cases of oblique astigmatism, the bias was nearly absent for both AR (−0.015 D) and CR (−0.079 D). Because the number of cases with oblique astigmatism component was small in our cohort, analysis of J45 is clinically meaningless (Fig. 2). In patients who had cylinder 0.75 D or more, the axis differences were relatively small. Only 23.0% and 3.8% of patients were outside 20° compared to AR and CR, respectively (Table 2). The relative difference of the astigmatism axis may be attributed to the following reasons: first, the wavefront aberrometer used in this study is a hand-held device, which makes it more vulnerable to misalignment during measurement. Similarly, shaking of the operator's hand during measurement may also contribute to inaccuracy. Finally, most of our subjects were children, so head tilting during measurement could explain poor agreement of astigmatism component. Third, ophthalmologists tend to do measurements at 180° or 170° rather than 175° or 173°.
Our study has some limitations. First, the sample size was relatively small, and most of the participants were young children. Older children or adults may have higher levels of agreement with CR. Second, none of the participants had other ophthalmic diseases. Thus, we could not determine the accuracy of the hand-held wavefront aberrometer in various clinical situations, such as cataract, corneal, and retinal disorders. Moreover, we measured the refractive errors once using the wavefront aberrometer, thus, it was not possible to test repeatability. Further prospective studies with larger sample sizes are needed to confirm wavefront aberrometer repeatability.
In conclusion, the hand-held wavefront aberrometer offers reliable information regarding refractive errors. Measurements made with the device did not differ significantly from those obtained by postcycloplegic AR and CR, especially in SE. However, the wavefront aberrometer showed significant differences in J0 vector component. Therefore, possible errors in cylinder measurement should be considered when measuring refractive errors using the hand-held wavefront aberrometer. This device uses wave-front technology when measuring the refractive error, and the OVITZ P10 (0.7 kg) is smaller and lighter than a spot vision screener (3.232 kg) and plusoptiX S12 (1.1 kg). It is not restricted by space, and is less affected by the patient's position. This is especially helpful for patients who have ambulation or postural disabilities that make traditional measurements difficult to obtain. Moreover, this device may be a good tool for screening large numbers of children at their schools with low cost and minimal training. Such examinations could trigger referral to ophthalmologists for actual eyeglass prescriptions, and thereby overall improve early detection of refractive errors in young children. Further, the device may be useful for physicians in low-income countries where medical space is limited.
Acknowledgements
The authors would like to extend our thanks to Felix Kim for providing the OVITZ P10 device. We also thank Geunyoung Yoon at University of Rochester for scientific advice.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.