

Horner's syndrome, first described by Johann Friedrich Horner in 1929, is characterized by the classic triad of miosis, ipsilateral blepharoptosis, and facial anhidrosis [1]. It can be caused by a viral infection, trauma, carotid dissection, or a tumor which interrupts the sympathetic innervation to the eyes and ocular adnexae [1]. Although the syndrome usually manifests by itself, it occasionally presents with other conditions such as ipsilateral abducens nerve palsy or herpes zoster ophthalmicus [2,3]. Many researchers have described the concurrence of Horner's syndrome and ipsilateral abducens nerve palsy [4-6], and the underlying causes were primary or metastatic tumors in the cavernous sinus, sphenodial sinus cyst, carotid aneurysm, or viral infections [2,3,7,8].
Herein, we describe a case of Horner's syndrome associated with contralateral abducens nerve palsy, which has not been previously reported. Diverse manifestations involving both eyes with other neurologic symptoms were caused by zoster meningitis and were successfully treated with anti-viral medication. To the best of our knowledge, this is the first description of this association.
Case Report
A 55-year-old woman presented with diplopia that had developed 12 days prior. The diplopia was preceded five days earlier by malaise and two days earlier by tingling sensation and pain in the right shoulder. The paresthesia spread along the whole right arm, and then arm weakness developed. Three days after the occurrence of paresthesia, the patient developed multiple painful vesicular eruptions on the right shoulder. After three more days, the tingling sensation involved the right lower leg.
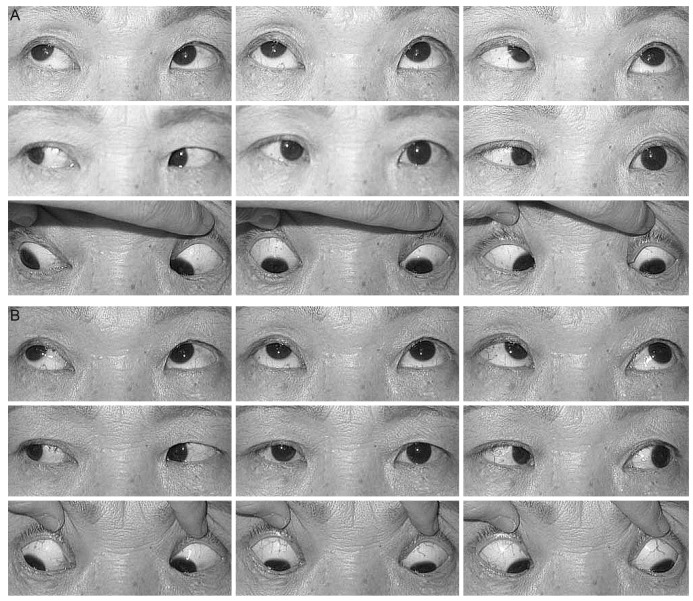
On presentation, she was found to have 35 prism diopters of esotropia, which worsened on left gaze at distance and near in the primary position. There was an abduction limitation in the left eye (Fig. 1A). The pupils were isocoric and reactive in both eyes. Visual acuity, the margin-reflex distance, levator function of the eyelid, anterior segments and fundi were normal in both eyes. The ocular and medical histories were unremarkable.
On neurological examination, right upper extremity strength was decreased to Medical Research Council grade II. Electromyography revealed a right C4 and C5 radiculopathy. Sensation was also decreased in the right C3 to C5 dermatomes. Although mental status was intact and brain magnetic resonance imaging (MRI) was normal, an analysis of cerebrospinal fluid (CSF) showed pleocytosis of 26 cells/mm3 and immunoglobulin (Ig) G varicella zoster virus (VZV) antibody. IgG and IgM VZV antibodies were detected in the serum as well. The patient was diagnosed as having zoster meningitis and was admitted for antiviral treatment. Acyclovir was administered intravenously and analgesics by mouth. With treatment, the skin lesions and shoulder weakness improved within one week.
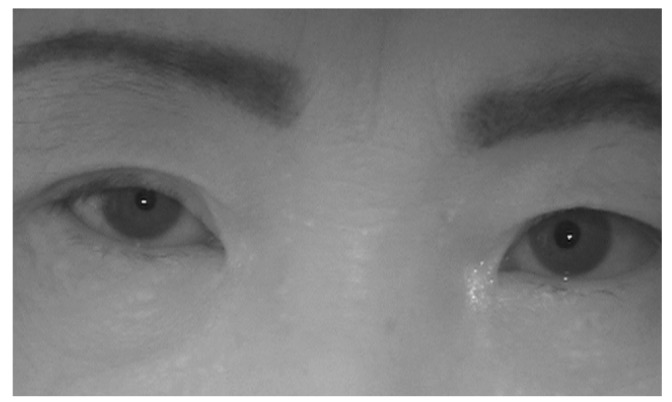
On the 14th day after admission, she newly developed right blepharoptosis. The marginal reflex distance 1 was 1.5 mm in the right eye and 3.5 mm in the left eye. The levator function was 12 mm in both eyes. The patient complained of hemifacial anhidrosis on the right side. Pupils were reactive in both eyes, however were anisocoric with the pupil size of 3 mm in the right eye and 4 mm in the left eye in light. Anisocoria increased in the darkness to 3 mm in the right eye and to 4.5 mm in the left eye (Fig. 2). She was diagnosed as having Horner's syndrome in the right eye. There was no change in the abduction limitation of the left eye. By the 22nd day, the motor and sensory functions recovered considerably and the patient was discharged.
When she returned to clinic one month after discharge, she demonstrated improvement of the abduction limitation in the left eye (Fig. 1B), but anisocoria and blepharoptosis were still persistent.
Six months after discharge, the abduction limitation and diplopia were completely restored. Anisocoria, blepharoptosis, and hemifacial anhidrosis resolved. The only remaining symptom was a mild paresthesia of the right arm.
Discussion
When Horner's syndrome is associated with ipsilateral sixth nerve palsy, the condition strongly implies a posterior cavernous sinus lesion [6,7]. However, the present case developed a contralateral abducens nerve palsy associated with Horner's syndrome, which has not been previously reported. Unlike the ipsilateral condition, it is not easy to explain the coexistence of Horner's syndrome and a contralateral abducens nerve palsy with a single localized lesion because the pathways of the oculosympathetic nerve and the contralateral abducens nerve are distant from each other. The present case had additional multiple neuronal involvements including the sensory and motor systems, as well as meninges. Furthermore, the sensory symptoms presented in multiple dermatomes of both the upper and lower extremities. Thus, it is difficult to confine the lesion.
Among diseases causing multiple neurological disorders, we reached the diagnosis of zoster meningitis. The clinical manifestations of herpes zoster such as painful eruptions, paresthesia, and arm weakness were helpful clues. Diagnosis was based on CSF pleocytosis and the presence of IgG VZV antibodies in CSF [9]. Brain MRI findings were normal, but consistent with previous reports [10]. The therapeutic effects of antiviral medication also supported the diagnosis.
When a patient presents with ophthalmoplegia, facial paralysis, and motor dysfunction, peripheral neuromuscular diseases such as Guillain-Barre syndrome, particularly Miller Fisher syndrome, should be ruled out [11]. The diagnosis of Miller Fisher syndrome was excluded for five reasons. Firstly, paresis of extraocular muscles in Miller Fisher syndrome is typically bilateral and accompanied by ataxia and areflexia. However, our patient did not demonstrate areflexia or ataxia, and only the abduction was limited unilaterally. Secondly, she developed right arm weakness accompanied by vesicular skin eruptions which also favors zoster meningitis rather than Miller Fisher syndrome. Thirdly, ataxia in Miller Fisher syndrome consists of a lack of voluntary coordination of muscle movements, but the arm weakness in our patient was muscular paralysis. Fourthly, combined anhidrosis also implies sympathetic dysfunction of Horner's syndrome. Lastly, CSF study revealed pleocytosis commonly seen in viral meningitis, not albuminocytological dissociation in Miller Fisher syndrome. Therefore, Horner's syndrome fits this case better than Miller Fisher syndrome.
The presence of the zoster meningitis explains the mechanism of multiple neuronal involvements. In zoster meningoencephalitis, VZV can reach various areas of the central nervous system through meninges and causes diffuse neuronal damage [12]. VZV may lead to clinical manifestations such as headache, malaise, pyrexia, nerve palsies, paresthesia, hemiplegia, and even Horner's syndrome [13]. Generally accepted pathogenesis of VZV includes a direct cytopathic effect on neural tissue, an allergic reaction of the nerve to the virus, and an occlusive vasculitis induced by the virus [13].
In conclusion, we suggest that viral infection should be considered with a high priority in the diagnosis of multiple neuronal dysfunctions. In particular, if neurological signs or symptoms manifest in both eyes, systemic as well as central nervous lesions should be ruled out. The common pathogen might be herpes simplex virus or VZV. The clinical findings of the present case may be helpful in diagnosing patients who present with several neuronal involvements.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






