Postoperative Stabilization of the Strabismic Angle in Intermittent Exotropia
Article information
Abstract
Purpose
To analyze the postoperative strabismic angle for five years or more and to investigate when the angle stabilized in intermittent exotropia.
Methods
We retrospectively reviewed the clinical records of 89 patients who had undergone surgery for intermittent exotropia. The postoperative strabismic angles measured were analyzed at one-year intervals up to five years postoperatively. We divided them into two groups according to their age at the time of surgery. Group 1 was less than 5 years of age, while Group 2 participants were 5 years of age or older.
Results
For our 89 total patients, average exo-angles were 7.8 ± 7.26, 7.9 ± 7.51, 9.5 ± 7.05, 10.1 ± 6.87, and 9.4 ± 6.90 prism diopters at one, two, three, four, and five years postoperatively, respectively. Average exo-angles between postoperative year one and year three, as well as between postoperative year two and year three, were statistically significant (p = 0.015, 0.022). However, the angles were not statistically significant between postoperative year three and year four or between years three and five, respectively (p = 0.707, p = 0.948). The stabilization characteristics of the angle were somewhat different according to age group. In Group 1, the average exo-angle in postoperative years one and three were statistically significant (p = 0.016), but the angle in the same period was not statistically significant in Group 2 (p = 0.203).
Conclusions
There was no significant interval change after three years postoperatively in intermittent exotropia, but if the patient's age at surgery was 5 years or higher, no significant change of exo-angle was found following postoperative year one in this study.
Intermittent exotropia is the most prevalent type of exotropia in childhood and therefore remains a widely studied disease. Numerous studies of postoperative success rate and recurrence rate of intermittent exotropia have been conducted. Reported success rates of intermittent exotropia were approximately 50% to 80%. There appears to be a consensus regarding the definitions of success. However, the follow-up period for judgment of success is variable among authors, ranging from 1 to 10 years (Table 1) [1-10].
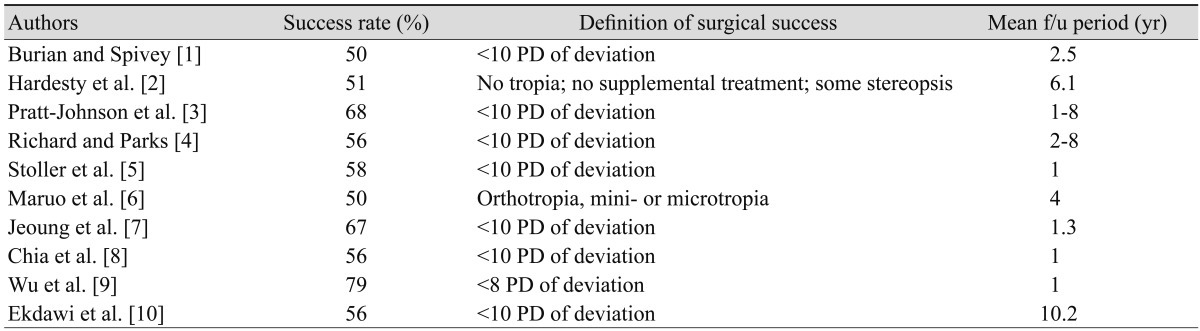
Previous reports of surgical success rates of intermittent exotropia
Therefore, the length of time that clinicians should follow-up patients after surgery for treatment of intermittent exotropia is questionable. This study was conducted to investigate the long-term changes of strabismic angle (up to five years after surgery) and the pattern of postoperative stabilization of strabismic angle according to the age at the time of surgery and also to suggest a reasonable follow-up period for intermittent exotropia after surgery.
Materials and Methods
We retrospectively reviewed the medical records of patients who underwent surgery for treatment of intermittent exotropia between 2002 and 2005 at Korea University Medical Center. Surgery was performed by only one surgeon (SHK). Principles outlined in the Declaration of Helsinki were followed in this study, and approval was obtained from the institutional review board of Korea University Medical Center.
Patients were excluded if their follow-up period was less than five years after surgery and if they had undergone re-operation for recurrence or consecutive esotropia. Participants who had other ocular or neurologic abnormalities were also excluded. Initially, we collected data from 130 patients; 24 were excluded because their follow-up periods were less than five years. Sixteen additional people were also excluded because they required re-operation (5 for consecutive esotropia and 11 for recurrent exotropia). One patient who underwent resection and recession was also excluded. Finally, we included and analyzed the data of 89 patients.
The alternative prism cover test was used to measure the strabismic angle, and strabismic angles measured at a distance of 6 meters were collected annually from postoperative year one through year five. To create a standard, we made four pairs of the angle on the basis of postoperative year three; postoperative years one through three, postoperative years two through three, postoperative years three through four, and postoperative years three through five. Each pair was analyzed to determine if there were statistically significant differences. Results of the preoperative sensory test (Vectographic projector test, Reneau, France) were also collected.
We divided the patients into two groups and analyzed the angle of difference according to age. Patients in Group 1 were 4 years of age or younger. Patients in Group 2 were older than 5 years of age. Changes of postoperative strabismic angles and patterns of stabilization were analyzed for each group and compared among the two groups. Continuous data are presented as a mean ± standard deviation, and categorical data are shown as counts and percentages. Comparisons of each pair of strabismic angles were completed using the Wilcoxon rank sum tests. The threshold of significance was set at p = 0.05. All statistical analyses were performed using the SPSS ver. 12.0.1 (SPSS Inc., Chicago, IL, USA).
Results
We included 89 patients in our study. Forty-two patients (47%) were male, and forty-seven (53%) were female. The mean age at surgery was 6.6 ± 2.44 years (range, 3 to 15 years). Group 1 included 24 (27%) patients, and Group 2 contained 65 (73%) patients. The basic type, which was defined when the difference between the distant and near strabismic angles was within 10 prism diopters (PD), was the most common (84%). Seventy-three (82%) patients underwent bilateral lateral rectus recession, and 16 (18%) received unilateral lateral rectus recession. These differences are summarized in Table 2. Before surgery, every patient showed unilateral or alternate suppression upon sensory tests. However, none of the patients showed suppression after one month postoperatively.
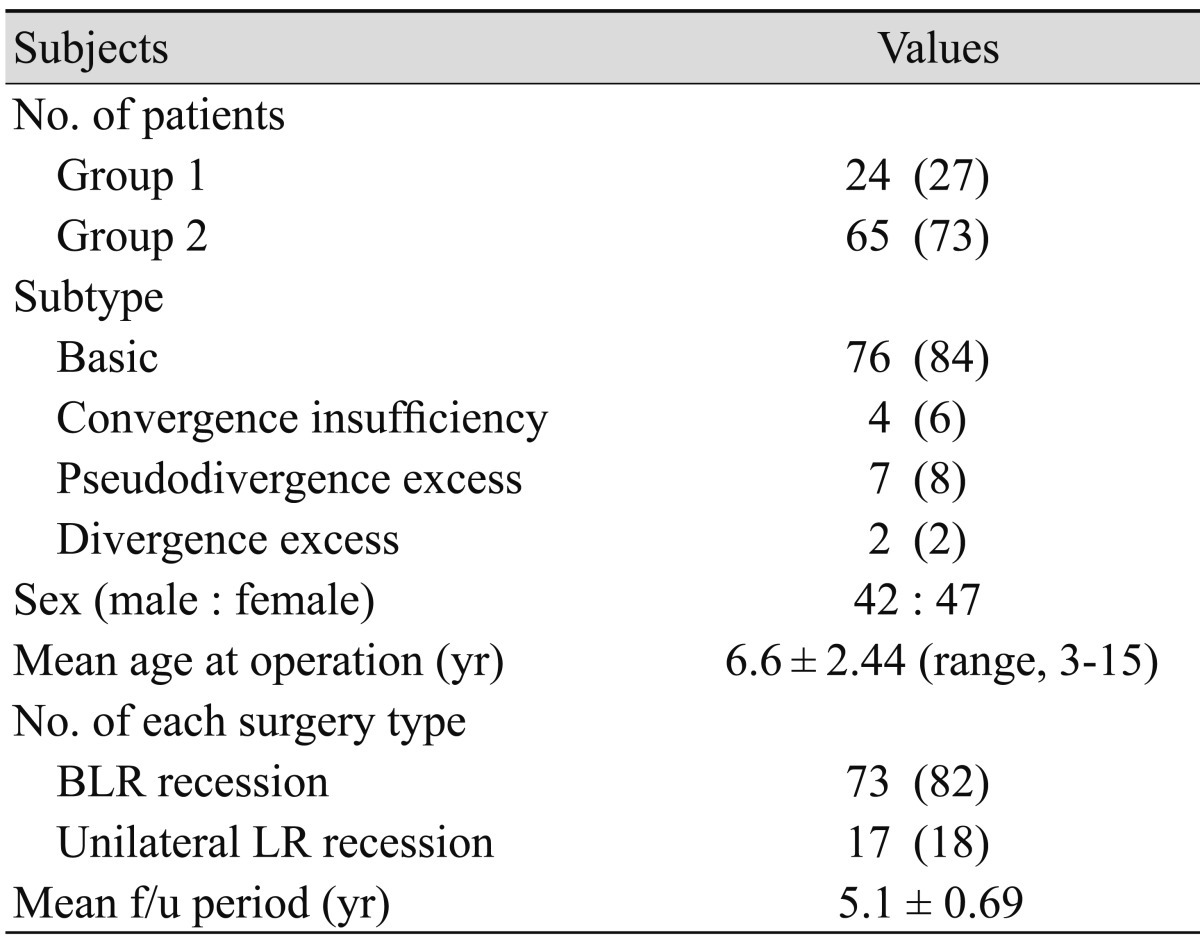
Clinical characteristics of the patients
Average strabismic angles measured annually from postoperative years one through five years were 7.8 ± 7.26, 7.9 ± 7.51, 9.5 ± 7.05, 10.1 ± 6,87, and 9.4 ± 6.90 PD, respectively (Table 3 and Fig. 1).

Postoperative strabismic angle (prism diopter) annually in the two groups
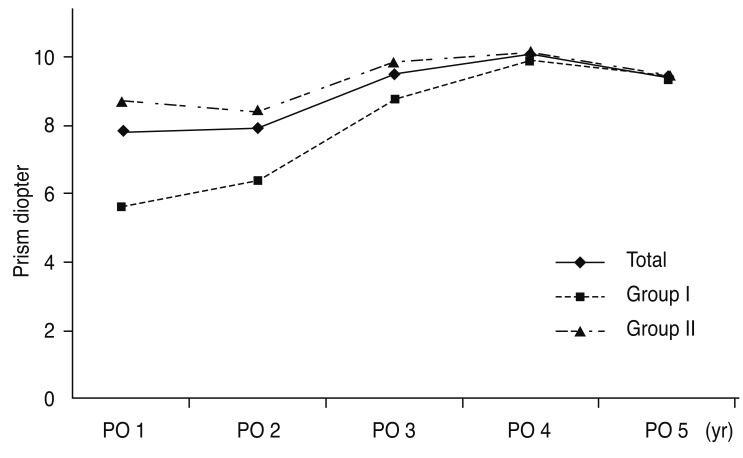
Curves of mean exo-deviation measured annually after surgery. PO = postoperative.
The p-values for the four pairs of postoperative strabismic angles are listed in Table 4. For all patients, statistically significant differences were observed between years one and three and years two and three postoperatively (p = 0.015, 0.022, respectively). However, no significant difference was observed between three years and four years or three years and five years postoperatively (p = 0.707, 0.948). In Group 1, the pattern was similar for all patients. The p-values between one year and three years and also between two years and three years postoperatively were 0.016 and 0.046, respectively. However, p-values between three years and four years and also three years and five years postoperatively were 0.767 and 0.794, respectively. In Group 2, there were no significant differences for all four pairs of strabismic angles (p = 0.203, 0.138, 0.888, and 0.939, respectively).

Statistical results of each pairs of postoperative year (p-values)
Furthermore, we calculated the amounts of exotropic drift for each group. We set the starting point as postoperative day one and the final ending point as five years postoperatively. The esotropic angle measured the first day following surgery was 4.29 PD for all patients (Group 1, 4.33 PD; Group 2, 4.28 PD). During the first two years after surgery, 89 percent of exotropic drift occurred for all patients; however, the portion of exotropic drift was smaller in Group 1 than in Group 2, even though there was no statistical significance (77.6% vs. 93.4%, p = 0.323). Results are summarized in Table 5 and Fig. 2.

Amounts of exotropic drift during the first year, first two years, and total five years (prism diopter)

Graphs of the amounts of exotropic drift during the first two years and the total five years.
Discussion
This study investigated the changes of strabismic angle measured annually after surgery and the pattern of stabilization of angle according to the patient's age at surgery. In this study, for all patients, we observed no significant change of strabismic angle after postoperative year three. In particular, patients in Group 2 (who underwent surgery after 5 years of age) showed no significant change of strabismic angle after the first postoperative year. Some previous reports concluded surgical success during a follow-up period of approximately one year [5,8,9]. Based upon our study, when the age at surgery was older than 5 years, one year was a sufficient amount of time to conclude surgical success because there was no significant change of angle after postoperative year one in Group 2 in our study.
Advocates of early surgery for treatment of intermittent exotropia before age 4 suggest that it yields better results compared with later surgery; however, reoperation rates, risk of developing amblyopia and loss of fusion are greater in the younger age group [11-13]. We reserved surgery in this age group for patients in whom rapid loss of control was documented or when intermittent exotropia has deteriorated to constant exotropia. Ju et al. [14] reported that if the age at surgery was younger, a larger eso-deviation was found the next day after surgery, and the amount of exotropic shift was also larger in the younger group. Edelman et al. [15] stated that an age younger than 4 years and immaturity of visual function were risk factors for consecutive esotropia. In our study, for patients in Group 1 in whom surgery was performed before 4 years of age, the amount of exotropic shift was larger and required a longer follow-up period of at least three years for the angle to become stabilized, even though total exotropic shifts for five years were not different (13.8 PD, 13.4 PD for Groups 1 and 2, respectively).
According to Scott et al. [16], during the first six weeks after surgery to treat exotropia, there was a substantial exotropic drift that stabilized and remained fairly constant during the two-year follow up period. The average additional amount of drift after two postoperative years ranged from 6 to 11 PD. Hahm et al. [17] reported the occurrence of remarkable exotropic drift during the first two years after surgery. A total 17.25 PD exotropic drift occurred in the entire five-year postoperative period, while 14.55 PD was recorded in the first two years. We set three postoperative years as the reference value because we thought that there may be abundant change of the angle within the first two postoperative years.
We further calculated the mean angle of deviation for all patients measured immediately on postoperative day one, which was 4.3 PD esodeviated in both groups. This finding reflects intentional surgical overcorrection for prevention of recurrence. The amount of exotropic drift for two years after surgery was 12.2 PD in our study. Five years after surgery, mean exotropic drift was 13.7 PD. Grossly, 90% of exotropic drift occurred in the beginning of the two-year period after surgery. Comparison with previous reports showed similar results.
There is a lack of consensus regarding an appropriate follow-up period for stabilization of the strabismic angle in intermittent exotropia. Hatsukawa [18] observed exotropic drift up until four years after surgery, and Nakagawa [19] reported exotropic drift until three years after surgery. Kordic et al. [20] found a 7 PD exotropic shift in the first postoperative year and an additional approximately 6 PD exotropic shift over the next average 12 years. In our study, we found approximately 12.1 PD, a much larger amount of exotropic shift, in the first postoperative year alone.
In summary, in this study, no statistically significant changes of strabismic angle were observed at approximately three years postoperatively, and stabilization of the strabismic angle was achieved at that time. However, in patients over 4 years of age who underwent surgery, stabilization of the strabismic angle was achieved earlier than in Group 1 patients. Therefore, it is necessary to follow-up with patients for at least three years after surgery for intermittent exotropia, particularly during at least the first year if surgery was performed after five years of age.
Notes
No potential conflict of interest relevant to this article was reported.