Clinical Outcomes of Cyclosporine Treatment for Noninfectious Uveitis
Article information
Abstract
Purpose
To assess the clinical outcomes of cyclosporine treatment for noninfectious uveitis.
Methods
A retrospective review of medical records was completed for 182 noninfectious uveitis patients who were treated with cyclosporine between January 2001 and August 2010. Data was obtained relevant to demographic characteristics, anatomic classification, and laterality of uveitis, associated systemic disorder, dosage of cyclosporine and prednisolone, usage of other immunosuppressive drugs, visual acuity (VA), control of uveitic activity, and adverse effects during the cyclosporine use.
Results
Uveitic activity was controlled to a level of minimal inflammation in 89.0% and completely in 78.6% of patients by the median duration of 49 and 98 days, respectively. Prednisolone-sparing (dose ≤10 mg) control of inflammation equal to or less than the minimal activity was achieved in 75.3% of patients. VA was aggravated more than 0.2 logarithm of the minimum angle of resolution in 17.3% of eyes in spite of cyclosporine treatment for the mean follow-up of 698.4 days. Dose reduction and cessation of cyclosporine was required only in 3.3% and 9.3%, respectively, due to the intolerable toxicity, although 44.0% of patients experienced mild to moderate adverse effects.
Conclusions
Cyclosporine combined with corticosteroids or other immunosuppressive drugs as needed is an effective treatment for noninfectious uveitis, thus minimizing the adverse effects of corticosteroids and other toxic drugs. However, careful monitoring for the toxicity of cyclosporine is needed, because a small group of patients cannot tolerate its toxicity.
Cyclosporine is an 11-amino acid cyclic peptide produced by fungi such as Beauveria nivea in nature. Cyclosporine exerts immunosuppressive effects through binding to cyclophilin of T-lymphocytes. The cyclosporine and cyclophilin complex inhibits calcineurin that activates the downstream cascades required for the transcription of interleukin-2, CD40 ligand, and Fas ligand, all of which are necessary for proper immune function [1].
Cyclosporine use for uveitis was first reported by Nussenblatt et al. [2] in 1983, and first applied clinically for renal transplantation in 1978 [3]. Afterwards, many studies ascertained the efficacy of cyclosporine in idiopathic uveitis, Vogt-Koyanagi-Harada disease, birdshot retinochoroidopathy, serpiginous choroiditis, and multifocal choroiditis and panuveitis, as well as in cases resulting from Behcet disease. However, only a few studies were performed in randomized, controlled, clinical trials, while most were retrospective case series [4-21].
In Korea, however, only two case series are currently available for the result of cyclosporine use in endogenous uveitis, where each treated only 15 patients for a rather short period of six to 18 months [22,23]. Thus, we present the long term results from a large group of Korean patients with regard to cyclosporine use for treatment of endogenous uveitis.
Materials and Methods
A list of patients for whom cyclosporine was prescribed to manage endogenous uveitis was extracted from the database of Seoul National University Hospital between 2001 and 2010. Two hundred patients with endogenous uveitis were managed with cyclosporine during the period and 18 patients were excluded from the study since cyclosporine treatment was started at other clinics. A retrospective review of medical records was completed for 182 noninfectious uveitis patients who were treated with cyclosporine between January 2001 and August 2010.
Cyclosporine was used when corticosteroids were insufficient to control uveitic activity, corticosteroid side effects were anticipated because of long-term use of high dose, or other immunosuppressive treatment failed to suppress the patient's inflammation. Cyclosporine was administered at a dose of ≤5 mg/kg/day, and the dose was adjusted according to uveitic activity following a tapering of corticosteroids. Adverse effects were regularly monitored with reports of a patient's discomforts, blood pressure, complete blood count with differentiation, renal function, liver function, and serum electrolyte as recommended [24].
Data was obtained relevant to demographic information, anatomic location, and specific diagnosis of uveitis. Moreover, we took note of systemic disorder, laterality of the inflammation, dosage of cyclosporine and prednisolone, usage of other immunosuppressive drugs, visual acuity (VA), uveitic activity before and after treatment, and adverse effects to the time when cyclosporine was discontinued or the last follow-up was reached. Uveitic activity was classified as "inactive", "slightly active", or "active", where any active posterior uveitis was noted as "active", while "slightly active" meant trace cells in the anterior chamber or the vitreous, or a trace haze of the vitreous [25]. If both eyes were involved, the uveitic activity in a more severe eye was recorded.
Averages and frequencies were calculated for each variable, while Kaplan-Meier survival analysis was applied for time to an inflammation control to "slightly active" or "inactive", and for time to a cessation of cyclosporine due to adverse effects. Decimal VA was converted into logarithm of the minimum angle of resolution (logMAR) for calculation. SPSS ver. 17.0 (SPSS Inc., Chicago, IL, USA) was employed for statistical analyses.
This study was approved by the Institutional Review Board at Seoul National University Hospital and adhered to the tenets of the Declaration of Helsin ki.
Results
The mean age of the patients was 44.6 ± 12.3 years (range, 17 to 77 years) and 99 patients (54.4%) were male. The mean duration of cyclosporine use was 698.4 ± 705.8 days (range, 30 to 3,303 days). Anatomic classification and specific diagnosis of uveitis treated with cyclosporine in our study are presented in Table 1. Panuveitis and Behcet disease-related uveitis were the most common anatomic location (74.2%) and specific diagnosis (48.4%) of uveitis, respectively, while panuveitis present in Behcet disease was the most common specific disease entity (40.7%) treated with cyclosporine. One-hundred twenty-three patients (67.6%) in our study had uveitis in both eyes.
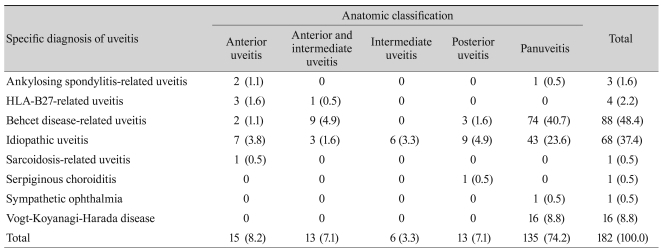
Anatomic classification and specific diagnosis of uveitis treated with cyclosporine
Cyclosporine was started at a mean dose of 164.2 ± 51.3 mg (range, 50 to 300 mg) together with prednisolone (mean, 19.5 ± 13.1 mg; range, 0 to 60 mg) in 161 patients (88.5%) and other immunosuppressive drugs in 46 patients (25.3%). Immunosuppressive drugs used before commencing cyclosporine included: azathioprine in 12 patients (6.6%), colchicine in six patients (3.3%), methotrexate in three patients (1.6%), and a combination of azathioprine and colchicine in three patients (1.6%); of these 24 patients, 18 patients continued their immunosuppressive treatment or changed to a drug other than cyclosporine. The mean dose of cyclosporine at the time of discontinuation or the last follow-up was 126.9 ± 61.5 mg (range, 25 to 300 mg). Ninety-one patients (50.0%) were still taking cyclosporine at the last follow-up, while 61 patients (33.5%) discontinued use and 30 patients (16.5%) were missing, where the mean duration of cyclosporine use was 905.2 ± 789.0 days (range, 122 to 3,303 days), 564.6 ± 585.8 days (range, 30 to 2,579 days), and 343.5 ± 406.6 days (range, 30 to 1,736 days), respectively. Adverse effects were the reason for cyclosporine discontinuation in five of 61 patients.
Uveitic activity was controlled to a level equal to or less than "slightly active" in 89.0% of patients by the median time of 49 days (range, 0 to 945 days; cyclosporine was added to one patient with "slightly active" uveitis), where 35.2%, 71.6%, and 87.0% of patients achieved this level of inflammation by the first one, three, and six months, respectively. The mean doses of cyclosporine and prednisolone were 166.7 ± 52.3 mg (range, 50 to 300 mg) and 15.9 ± 10.5 mg (range, 0 to 60 mg), respectively, while 30.8% of patients were taking other immunosuppressive drugs. "Inactive" uveitis was shown in 78.6% of patients by the median time of 98 days (range, 7 to 1,146 days), where 16.1%, 47.6%, and 73.4% of patients achieved this complete resolution of uveitis by the first one, three, and six months, respectively. The mean doses of cyclosporine and prednisolone at the time of first "inactive" uveitis were 163.3 ± 52.4 mg (range, 50 to 300 mg) and 13.5 ± 9.2 mg (range, 0 to 50 mg), respectively, while 31.3% used other immunosuppressive drugs simultaneously. Achievements of these levels of uveitis resolution according to time were demonstrated from Kaplan-Meier survival analyses in Fig. 1. Corticosteroid-sparing (prednisolone dose ≤10 mg) control of inflammation equal to or less than "slightly active" was achieved in 75.3% of patients.
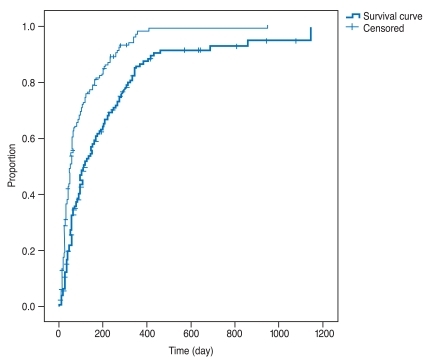
Kaplan-Meier survival curve showing the uveitis control against time. The upper curve denotes a level equal to or less than "slightly active" and the lower curve denotes a level of "inactive".
One-hundred ten patients who showed a control of inflammation equal to or less than "slightly active" had experienced recurrence of "active" uveitis after a median duration of 83 days (range, 10 to 546 days) from the time when "slightly active" states were achieved. At the recurrence of "active" uveitis, the mean doses of cyclosporine and prednisolone were 148.0 ± 55.7 mg (range, 0 to 300 mg; one patient experienced "active" uveitis after cessation of cyclosporine) and 8.9 ± 6.0 mg (range, 0 to 25 mg), respectively.
In the last medical records considered in our study, 82 patients (45.1%), 41 patients (22.5%), and 59 patients (32.4%) showed "inactive", "slightly active", and "active" uveitis, respectively. VA at the last follow-up was aggravated by more than 0.2 logMAR in 17.3% of eyes in spite of cyclosporine treatment during the study time.
Adverse effects were experienced by 44.0% of patients, which are tabulated in Table 2. Hyperglycemia was the most common adverse effects in 25.3% of patients, while nephropathy was observed only in two patients. Dose reduction and cessation of cyclosporine was required only in 3.3% and 9.3% of patients respectively, due to the intolerable toxicity. This result is visualized with Kaplan-Meier survival curve in Fig. 2.

Adverse effects of cyclosporine used for endogenous uveitis

Kaplan-Meier survival curve demonstrating the proportion of patients who needed a dose reduction or cessation of cyclosporine due to adverse effects.
Discussion
Cyclosporine was effective for endogenous uveitis by reducing a uveitic inflammation to "slightly active" in 89.0% of patients and to "inactive" in 78.6% of patients. Most patients achieved these effects by six months in 87.0% for "slightly active" and 73.4% for "inactive" uveitis. Only 17.3% of patients experienced visual loss of more than 0.2 logMAR at the last follow-up when considering the severity of uveitis that could not be managed with a sole treatment using corticosteroid.
Previous studies reported similar or inferior effectiveness of cyclosporine for ocular inflammatory disease compared to our study [2,6-9,12-14,17,20,21,26]. This disparity comes from the differences in outcome measures and the definition of success in uveitis control, thus making direct comparison between studies impossible. We did not consider maintenance of partial or complete resolution of inflammation when deciding a treat ment success, and included the patients who concurrently took other immunosuppressive drugs. Thus, our study showed superior effectiveness of cyclosporine in endogenous uveitis compared to the ones with a stricter measure of success [12,20,26]. As an input, we considered the uveitic activity based upon the eye with more severe inflammation when bilateral uveitis was encountered since systemic cyclosporine was applied to a patient, which, on the contrary, might decrease the success rate of cyclosporine.
The shortest duration of follow-up was 30 days in our study. We did not limit the follow-up time for exclusion, because the quickest time for a resolution of uveitis to "slightly active" or "inactive" was seven days. Since 9.9% of patients in our study used cyclosporine for less than three months, this fact may have decreased the rate of success or adverse effects observed in this study.
Overall, many patients (110 of 162 patients, 67.9%) experienced recurrence of "active" uveitis after achieving equal to or less than "slightly active" uveitis. This might be attributed not only to the reduced dose of cyclosporine and corticosteroids, but also to the limitation in sustained suppression of uveitis with cyclosporine or the clinical features of included uveitis.
Only a small group of patients in our study discontinued cyclosporine due to toxicity, which is superior to other studies that reported adverse effects with low-dose cyclosporine for ocular inflammation [17,20,21,27]. We used a protocol of relatively rapid cyclosporine dose reduction according to inflammation status, which might have also contributed the lower rates of toxicity. In addition, more adverse effects might be found in the 16.5% of missed patients, which also decreased the observed adverse effects.
The limitations of our study are obvious as it is a retrospective study. The usage of cyclosporine and other drugs were not controlled and compliance could not be assessed. The results may not be applied to a general population, because uveitis with worse prognosis tended to be included as a tertiary referral center. In addition, there might be disparities between retinologists in the grading of uveitic inflammation that could cause an error in data analyses.
In conclusion, cyclosporine combined with corticosteroids or other immunosuppressive drugs as needed is effective for endogenous uveitis, via minimizing the adverse effects of corticosteroids and other toxic drugs. However, careful monitoring for cyclosporine toxicity also is needed.
Notes
No potential conflict of interest relevant to this article was reported.