A Case of Central Retinal Artery Occlusion after Chiropractic Manipulation of the Neck
Article information
Abstract
Here we report a case of central retinal artery occlusion after chiropractic manipulation on the neck. A 49-year old man presented at the hospital because of sudden visual loss in his right eye after chiropractic neck manipulation. He had received chiropractic manipulation of the neck by a chiropractor eight days prior. When he first visited us, his best corrected visual acuity in his right eye was hand motion. A full ophthalmic examination was performed. There was cherry-red spot in the macula in his right eye. We performed a fluorescein angiogram and cervical color Doppler. The arterio-venous transit time in the fluorescein angiogram was delayed, and we detected stenosis of the right internal carotid artery with diffuse atherosclerotic plaques in the right common carotid artery. We prescribed ginko biloba extract (Tanamin). Three years after his first visit, the best corrected visual acuity of his right eye was 20 / 200.
With the great demand throughout the industrialized world for complementary and alternative medicine, chiropractic manipulation and spinal massage technique are becoming increasingly popular worldwide [1]. However, unexpected, albeit rare, side effects from chiropractic manipulations have also been reported. For example, less than one hundred cases of stroke from chiropractic manipulation have been reported since 1925 [1,2]. Five cases of central retinal artery occlusion following cardiac catheterization [3,4] and one case of central retinal artery occlusion after chiropractic manipulation on the neck have also been described [1]. Here we describe a patient with central retinal artery occlusion following chiropractic manipulation, which has not previously been reported in Korea.
Case Report
A 49-year old man was referred to us with painless sudden visual loss in his right eye. Eight days prior to his visit, he received chiropractic manipulation on his neck in a prone position for approximately 10 minutes to improve neck and shoulder stiffness. Immediately after rising, he was unable to see with his right eye. When he first visited our clinic, the best corrected visual acuity in the right eye was hand motion, while the left eye was at 20 / 20. Anterior segment examination was unremarkable, and the right eye had a relative afferent pupillary defect. There was cherry-red spot in the macula in his right eye (Fig. 1), and the arterio-venous transit time in the fluorescein angiogram was delayed (Fig. 2). A cervical color Doppler showed stenosis of the right internal carotid artery (Fig. 3) with diffuse atherosclerotic plaques in the right common carotid artery (Fig. 4). The right anterior communication artery was not visible by magnetic resonance angiogram (Fig. 5).
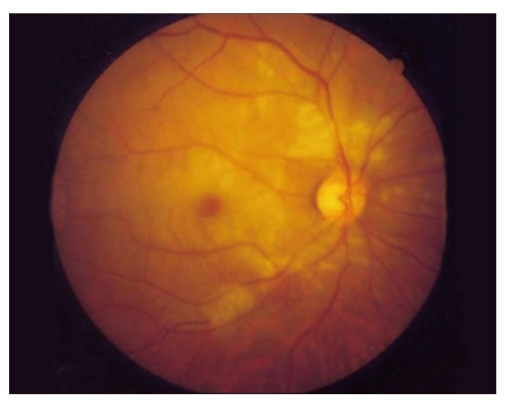
Fundus photograph of the right eye showed whitening and opacification of the retina with a cherry-red spot in the fovea.
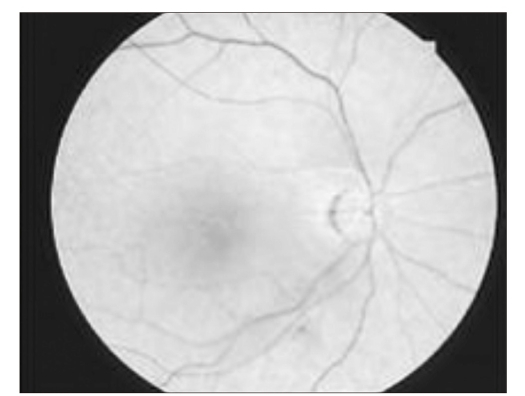
The fluorescein angiogram indicated that the right retinal artery was still poorly filled, 35.0 second after injection.
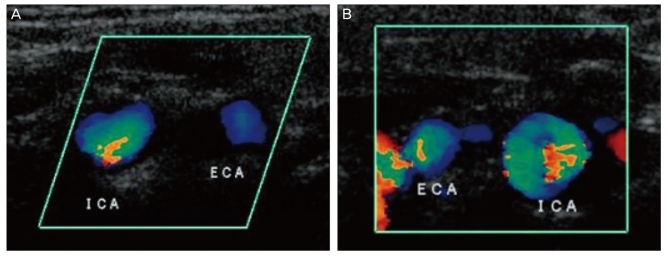
Cervical color Doppler showed that the right internal carotid artery (A) was narrower than the left internal carotid artery (B). ICA = internal carotid artery; ECA = external carotid artery.
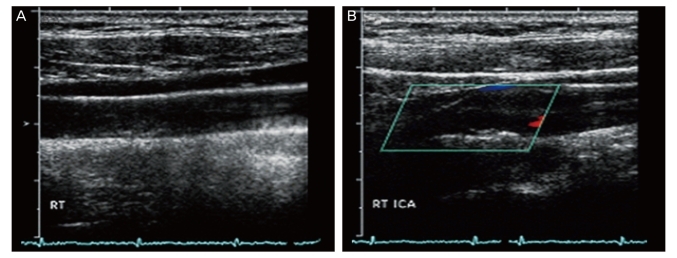
Cervical color Doppler showed diffuse atherosclerotic plaques in the right common carotid artery (A) and stenosis of the right internal carotid artery (B). RT = right; ICA = internal carotid artery.
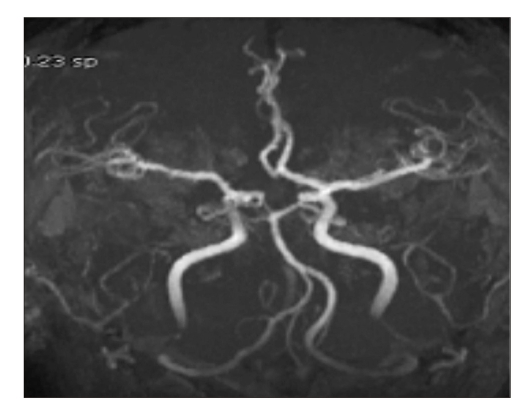
The right anterior communication artery was not visible by magnetic resonance angiography.
The patient had been taken hospitalization twice previously because of cerebral infarction. He has suffered from dysarthria, which is sequela of cerebral infarction. He has taken medicine for hypertension and diabetes mellitus for 5 years.
In our case of central retinal artery occlusion, the usual emergency efforts to restore retinal circulation such as ocular digital massage and anterior chamber paracentesis were not performed because eight days had already passed. We prescribed ginko biloba extract (Tanamin; Yuyu Pharmacy, Seoul, Korea), 3 tablets per day. Three years after the patient's first visit, the best corrected visual acuity of his right eye was 20 / 200.
Discussion
Chiropractic, a discipline founded by D. D. Palmer in 1895, attributes illness to incorrect alignment of spine and seeks to treat diseases by manual manipulation of the spinal vertebrae [1]. Approximately 10% of Americans consult chiropractors an average of seven to ten times per year, accounting for roughly 0.25 billion patients visit per year [1,5]. Despite the large number of treatment sessions, complications following chiropractic treatment have been largely ignored. Askey [6] reported six instances of hemiplegia immediately after spinal chiropractic massage, and Calverley and Millikan [7] and Millikan [8] described a total of seven patients who experienced contralateral paralysis after manipulation of the neck. Jumper and Horton [1] reported a case of central retinal arterial occlusion followed manipulation of the neck by a chiropractor.
Central retinal arterial occlusion (CRAO) often results in profound, permanent loss of vision and is frequently associated with systemic vascular disease [9]. The causes of CRAO include embolism, thrombosis, vasculitis, arterial spasm, arterial dissection, and hypertensive arteriolar necrosis [3]. Of these, embolism is by far the most common cause, and the major source of emboli is a plaque in the carotid artery [10]. The risk factors for arterial occlusive disease include hypertension, coronary artery disease, diabetes mellitus, hypercholesterolemia, and tobacco use [9-11].
Here, we reported on a patient with central retinal artery occlusion following chiropractic neck manipulation. We suspect that cervical manipulation by the chiropractor dislodged an embolus from an artherosclerotic plaque in the right common carotid artery, which was obstructing the right internal carotid artery.
In conclusion, before undertaking neck manipulation, chiropractors and other medical personnel should inquire about a history cervical vascular disease, especially in older patients. The carotid artery should always be handled gingerly in patients with known or suspected artherosclerotic disease.
Notes
This paper was presented in part at the 92nd annual meeting of the Korean Ophthalmological Society, November, 2004.
No potential conflict of interest relevant to this article was reported.