

Seborrheic keratosis (SK) is a common, benign, cutaneous tumor that is frequently seen on the trunk, extremities, head and neck of elderly people. The lesions typically begin as flat, sharply demarcated, brown macules. As they progress, they become polypoidal, with an uneven surface. The etiology of SK is unknown, although sun exposure, human papilloma virus (HPV), and epidermal growth factors (EGF) have been suggested as possible etiologies [1]. SK is usually divided into the following six histological subtypes: acanthotic, hyperkeratotic, adenoidal or reticulated, clonal, irritated, and melanoacanthoma variants [2].
We have only found one case of SK after surgery in the English medical literature. This is the first case of a irritated SK discovered at the incision site. We describe herein an 83-year-old woman with an irritated SK on her incision site after an external dacryocystorhinostomy (DCR).
Case Report
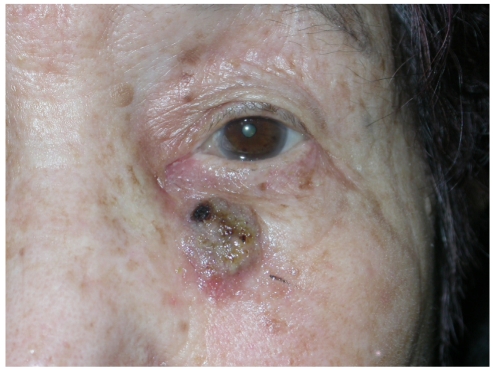
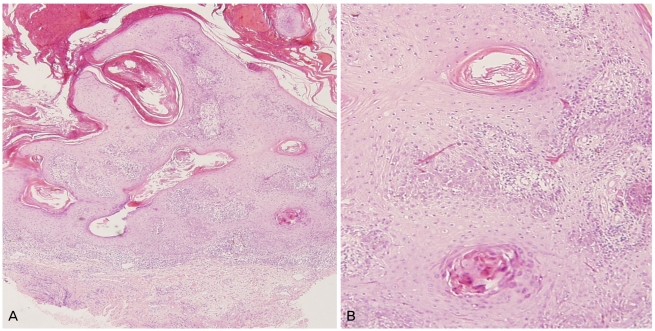
An 83-year-old woman presented with a complaint of epiphora from her left eye. She had no relevant general medical or ocular history, and took no medication. She had complete nasolacrimal duct obstruction, as evaluated by irrigation. She received external DCR with silicone intubation. Before the surgery, no skin lesions were observed at the incision site. The patient returned three months after surgery,complaining of a mass at her previous skin incision site. According to the patient's history, the mass had noticeably increased in size over the previous two months. Upon examination, a dome-like brown-to-black, polipoid, greasy surfaced elevation of 1×1.5 cm in diameter was observed (Fig. 1). A punch biopsy was performed for diagnosis, which demonstrated irritated SK with hyperkeratosis, basaloid cell proliferation, acatholysis with squamous eddies, and inflammatory infiltrates in the epidermis (Fig. 2). The patient received CO2 laser therapy. No recurrence had been noted after a six-month follow-up.
Discussion
SKs are the most common benign tumors in older individuals. The etiology of SK is unknown, although sun exposure, HPV, and EGF have been suggested as possible etiologies [1]. To date only one case of SK after surgery has been reported. Satterfield and Haas [3] reported a case of a postoperative localized eruption of SK. They hypothesized that the growth factor being induced by the healing graft site stimulated the appearance of the SK locally. In our patient, the SK also occurred postoperatively, and we think the EGF may have had a role in the development of SK on the incision site.
Histologic changes in SK after its irritation have been well documented by several other authors [4,5]. There are a few case reports describing the sudden, macroscopic transformation of irritated SK. Mochizuki et al. [6] reported a case of giant irritated SK that mimicked a verrucous carcinoma. Aydogan et al. [7] described a patient with an irritated SK that presented as a cutaneous horn. Our case shares many characteristics with those of previous cases, as the SK noticeably increased in size over several months. However, unlike the cases described before, our patient had no visible skin lesion at the incision site. We might hypothesize that in this case, the irritation being induced by the surgical incision stimulated very small or microscopic skin lesions at the incision site. Therefore surgeons need to check the patient's skin carefully for skin lesions on the incision site, and they should consider how to treat these lesions prior to surgery.
To our knowledge, this is the first reported case of a irritated SK found on a previous skin incision site. Therefore, we deemed it worthy of report.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






