Application of Intravitreal Bevacizumab for Circumscribed Choroidal Hemangioma
Article information
Abstract
We report 3 cases of circumscribed choroidal hemangioma (CCH) effectively managed with intravitreal bevacizumab. One patient (case 1) who had recurrent CCH (1.6 mm in thickness) with prior laser photocoagulation was treated with intravitreal bevacizumab alone. Two patients (case 2 and 3) who had CCH (2.4 mm and 2.2 mm in thickness, respectively) with recent visual impairment were treated with bevacizumab followed by photodynamic therapy (PDT). Ophthalmic evaluations included visual acuity, ophthalmoscopic examination, fluorescein angiography, ultrasonography, and optical coherence tomography. Patients were followed up for 6-9 months. After therapy, all patients showed improved visual acuity due to complete resorption of subretinal fluid and macular edema. Ultrasonography demonstrated a reduction of the thickness of CCH in case 1 and complete regression of the lesions in case 2 and 3. No patient showed tumor recurrence. Intravitreal bevacizumab, alone or in combination therapy with PDT, may be a useful alternative for the treatment of symptomatic CCH with subretinal fluid.
Circumscribed choroidal hemangioma (CCH) is an uncommon, benign vascular tumor manifesting as a discrete smooth, round, orange-red mass located posteriorly to the equator, mostly in the macular and peripapillary region.1 Although CCH is a benign lesion and is probably congenital, progressive enlargement and chronic exudation over decades may significantly compromise vision.2 Intraretinal edema and accumulation of subretinal fluid affecting the macular area account for decreased vision in most patients.3-5 The spontaneous course of an acutely decompensated hemangioma is generally unfavorable.6
Thus, many treatment modalities for symptomatic CCH have been introduced, including laser photocoagulation,4,5,7 cryotherapy,8 radiotherapy,9-12 transpupillary thermotherapy (TTT),13 and photodynamic therapy (PDT).14-17 However, these treatment options may cause additional, severe functional impairment.
Bevacizumab (Avastin, Genentech, Inc., San Francisco, CA) is a humanized monoclonal antibody to vascular endothelial growth factor (VEGF). Selective antibody blocking (anti-VEGF therapy) inhibits the formation of abnormal blood vessels and decreases vascular permeability.18 In an off-label manner, intravitreal bevacizumab has been used to treat various neovascular ocular pathologies,19,20 macular edema (ME),21,22 and revision of a filtering bleb.23 And, recent case studies have reported on the efficacy of bevacizumab for the treatment of vasoproliferative retinal tumors including retinal capillary hemangioma.24,25 From these observations, we thought that bevacizumab should offer the ideal qualities for the treatment of CCH with subretinal fluid. To our knowledge, this is the first report to apply bevacizumab in the treatment of CCH.
We here report a case of recurrrent CCH with prior photocoagulation that improved clinically after intravitreal bevacizumab and two cases of CCHs that showed visual and clinical improvement after combination therapy with intravitreal bevacizumab and PDT.
Case Report
Case 1
A 55-year-old man was initially referred at the age of 42 years because of decreased vision and submacular fluid that was thought to be related to a choroidal lesion centered inferior to the macula. Ophthalmic examination documented visual acuity of 1.0 OD and 0.3 OS. The fundus showed normal retina in the right eye and a pink choroidal tumor inferior to the macula, with accumulation of subretinal fluid into the macular area, in the left eye. A fluorescein angiography showed early preretinal patchy hyperfluorescence and patchy late staining of the tumor with some dye leakage into the submacular space. A clinical diagnosis of circumscribed choroidal hemangioma with exudative detachment was made. At presentation, a treatment with photocoagulation to the surface of the lesion had been administered in an attempt to foster resolution of the vision-impairing subretinal fluid. Two months later, visual acuity had improved from 0.3 OS to 0.8 OS and remained relatively stable for one year. Since then, follow-up was lost for thirteen years.
He visited again with a two-week history of decreased visual acuity in the same eye. The visual acuity had decreased to 0.3 OS. Ophthalmoscopic examination of the left eye revealed an elevated orange-red lesion inferior to the macula, with localized areas of retinal pigment epithelial rarefaction and clumping caused by prior photocoagulation. A serous detachment of edematous neurosensory retina extended from the lesion into the macular area. Ultrasonography revealed a domeshaped choroidal tumor 1.6 mm thick with high internal reflectivity. Optical coherence tomography (OCT) also demonstrated submacular fluid around the tumor.
After obtaining the patient's fully informed consent, we treated the lesion with intravitreal bevacizumab injection (1.25 mg in 0.05 mL in a tuberculin syringe). The injection was performed in a sterile fashion through pars plana using a 30-gauge needle after preparation with a topical anesthetic and placement of a lid speculum. Following injection, optic nerve perfusion was assessed by clinical examination with dilated ophthalmoscopy and topical antibiotics were used three times daily for one week.
At follow-up one month later, subretinal fluid around the tumor was not recognizable, and visual acuity had improved to 0.6 OS. Two months later, visual acuity was 1.0 OS, and B-scan ultrasonography showed a decrease of the tumor (Fig. 1). The tumor had not recurred during follow-up of eight months.
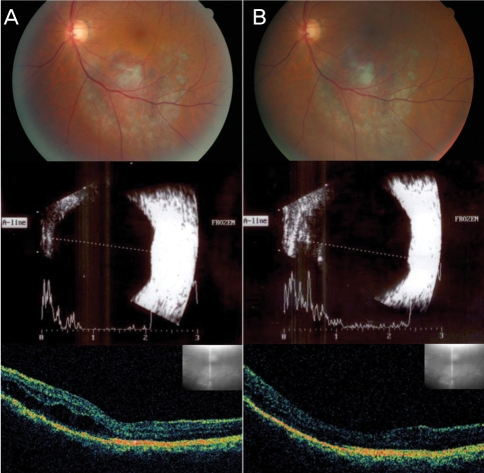
Case 1. (A) Recurrent choroidal hemangioma with submacular fluid, previously treated by photocoagulation, before intravitreal bevacizumab. Ultrasonography reveals a tumor thickness of 1.6 mm. Optical coherence tomography (OCT) demonstrates the presence of submacular fluid. (B) Two months after intravitreal bevacizumab. The hemangioma thickness is reduced on ultrasonography and the subretinal fluid around the tumor is absorbed on OCT.
Case 2
A 47-year-old woman was presented with a recent decrease in vision in her right eye. Visual acuity was 0.15 OD and 1.0 OS. The left fundus was normal. The right fundus showed an elevated, red-orange choroidal lesion superotemporal to the macula with a thin layer of subretinal fluid into the macular area. B-scan ultrasonography revealed a lesion with high internal reflectivity measuring 2.4 mm in thickness. Fluorescein angiography showed prearterial patchy filling of the tumor with late patchy staining and dye leakage into the subretinal space. The patient was clinically diagnosed as a CCH.
After obtaining fully informed consent, bevacizumab (1.25 mg in 0.05 mL in a tuberculin syringe) was injected. One week after the intravitreal bevacizumab, serous detachment had decreased and visual acuity had increased to 0.5 OD. At this time, PDT was administered. The patient received an intravenous infusion of 6 mg/m2 of verteporfin (Visudyne, Norvatis Ophthalomics, Hettlingen, Switzerland). Fifteen minutes after the start of the infusion (approximately five minutes after completion of infusion), laser light at 689 nm was delivered with an intensity of 600 mW/cm2 for 83 seconds (50 J/cm2). The diameter of the treatment spot was 5,200 µm which was based on the lesion size measured on the pretreatment fluorescein angiography. No additional safety margin was added to the diameter of the spot.
Two weeks after PDT, visual acuity had improved to 0.6 OD. B-scan ultrasonography at this time showed a marked reduction in the thickness of the tumor. There was no subretinal fluid, but the primary ophthalmoscopic appearance showed rarefaction of the retinal pigment epithelium at the tumor site. Three months after PDT, visual acuity had improved to 0.8 OD and the tumor was completely flat. However, RPE atrophy remained at the site of the original tumor (Fig. 2). There was no tumor recurrence at the six-month follow-up visit.
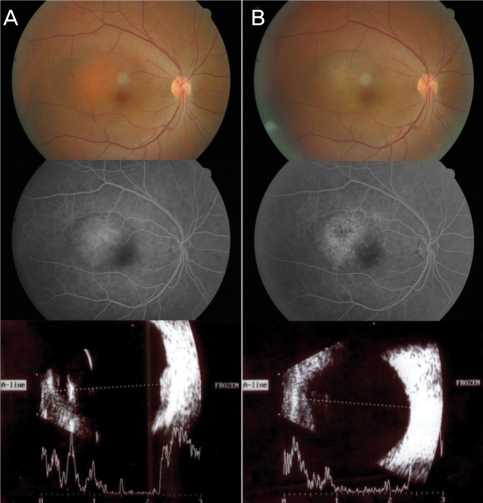
Case 2. (A) A red-orange choroidal hemangioma with submacular fluid. Fluorescein angiography shows late patchy staining of the tumor with some dye leakage into the submacular space and ultrasonography reveals a solid dome-shaped lesion 2.4 mm in thickness. (B) Three months after bevacizumab followed by photodynamic therapy. The hemangioma has flattened and shows pigmentary change by the retinal pigment epithelium atrophy. Fluorescein angiography reveals marked regression of the leakage into the macula and some hypofluorescence caused by pigmentary change. The tumor has regressed to a non-measurable thickness on ultrasonography.
Case 3
A 51-year-old man was referred for a 10-day history of decreased visual acuity in the right eye. Visual acuity was 0.06 OD and 1.0 OS. Fundus examination of the right eye showed an elevated, orange-red choroidal lesion that was contiguous with the optic nerve from approximately the 8-o'clock position clockwise to the 1-o'clock position. There was a serous detachment of the sensory retina that extended from the tumor into the macular area. Ultrasonography revealed a tumor thickness of 2.2 mm. The fluorescein angiographic features of the lesion were characteristic of hemangioma. Choroidal hemangioma with vision loss from associated submacular fluid was diagnosed.
After informed consent was obtained, intravitreal bevacizumab (1.25 mg in 0.05 mL) was injected. One week later, a decrease in subretinal fluid was noted. At this time, PDT was performed (laser spot size of 5,100 µm) using the same power and intensity as described in case 2 but not overlapping the optic nerve with the laser.
Two weeks after PDT, subretinal fluid was absent, and visual acuity was 0.15 OD. Three months after PDT, visual acuity had improved to 0.3 OD and the tumor had markedly regressed (Fig. 3). Nine months after treatment, the visual acuity remained 0.3 OD, and no tumor had recurred.
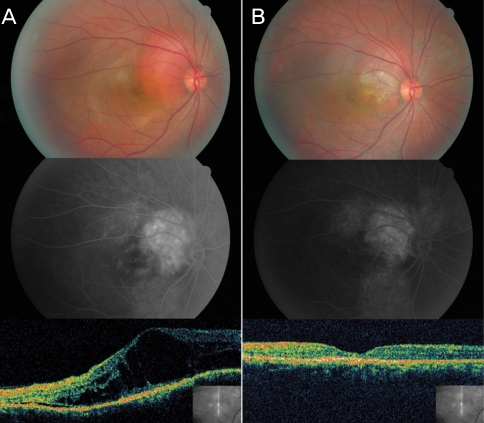
Case 3. (A) A red-orange choroidal hemangioma contiguous with optic nerve from the 8-o'clock position clockwise to the 1-o'clock position. A serous detachment around the tumor extends into the macula. Fluorescein angiography shows dye leakage into the submacular space and optical coherence tomography (OCT) demonstrates serous detachment around the fovea. (B) Three months after bevacizumab followed by photodynamic therapy. The tumor has flattened around the macula, without subretinal fluid. Fluorescein angiography shows no submacular leakage and diminished hyperfluorescence in the tumor. OCT shows nearly regular foveal anatomy.
Discussion
CCH is a benign intraocular hamartoma that can cause visual impairment by various mechanisms, such as transudative leakage, accumulation of subretinal fluid and serous retinal detachment with secondary photoreceptor damage as well as cystoids macular edema.3-5 Treatment is required only for patients with visual symptoms.3 In cases of small asymptomatic lesions, observation is recommended to detect any signs of progression, growth, or exudation.
Laser photocoagulation,4,5,7 cryotherapy,8 plaque radiotherapy,9 external beam radiotherapy,10 proton beam radiotherapy,11 TTT,13 and PDT14-17 have been proposed for the treatment of symptomatic CCH. These treatments are chosen variably depending on tumor size, location, and associated subretinal fluid.26 They have been shown to be beneficial in a number of cases.
However, these currently available treatments have limitations because of the invasiveness, lack of effectiveness, complications, or lack of precision with which the lesion can be treated. After laser photocoagulation, leakage from hemangiomas have recurred in more than 50% of patients and often have resulted to progressive visual loss.4,7 Radiation therapy or proton beam therapy may lead to complications such as cataract, radiation maculopathy or retinopathy, and an increased risk for development of osteosarcomas or soft tissue sarcomas.9-12 TTT induces chorioretinal atrophy in the treated area and is not beneficial in subfoveal lesions.13 PDT may also cause infrequent complication such as chorioretinal atrophy resulting from too intensified treatment.14,17
Meanwhile, bevacizumab has been approved for the treatment of metastatic colorectal cancer. It acts as an inhibitor of VEGF, potentially decreasing the permeability of the retinal vasculature.18 During recent years, intravitreal bevacizumab injection has been used in the treatment of ME associated with diabetic retinopathy, central retinal vein occlusion and neovascular age-related macular degeneration while reporting that adverse effects of these injections did not show any increase in the rate of potential ocular and systemic events.20-22 Other reports have shown intravitreal bevacizumab to be effective for the treatment of pseudophakic ME and radiation ME.27,28 With regard to management of intraocular tumor using bevacizumab, Kenawy et al.24 reported a patient with vasoproliferative retinal tumor, who showed visual and clinical improvement after this treatment. Wang et al.29 underlined that bevacizumab alone can lead to a reduction in the tumor-associated exudation, presumably by depleting endothelial fenestrae and altering intercellular adhesion molecules. On the basis of these observations, intravitreal bevacizumab was considered as an alternative to standard therapy in the first patient who had a small CCH with subretinal fluid recurrence after prior laser photocoagulation. Judging by the lack of complications in previous studies using intravitreal bevacizumab,18-22 the risk of adverse results in patients with CCH seemed low. This patient showed a marked improvement in visual acuity resulting from resorption of subretinal fluid and regression of the macular edema, which was maintained for eight months. Thus, we thought that bevacizumab should offer a new, effective approach to the treatment of CCH, even though the follow-up period was short and this case was a small tumor with recent subretinal fluid which may be considered good prognostic factor for vision recovery.
In many reports related to the management of CCH, treatments have been aimed primarily at decreasing tumor-associated leakage and subretinal fluid that cause visual symptoms. But, some investigators reported that an ideal treatment for CCH should achieve not only the regression of subretinal fluid, but also the occlusion of the vascular network of the tumor or its complete atrophy, thus inducing preservation, if not improvement, of the retinal function.14-17 And others reported that the persistence of abnormal vascular tissue can cause recurrence of subretinal fluid with progressive impairment of visual acuity.6,16 PDT allows selective photochemical destruction through free radical induced damage of vascular endothelial cells, while preserving normal retinal and neurosensory structures. Occlusion of targeted abnormal vessels results in vascular tissue fibrosis and secondary tumor regression. Schmidt-Erfurth et al.30 demonstrated complete and irreversible vascular occlusion of experimental choroidal tumors after PDT. Thus, for recent several years, PDT has been accepted as the most effective treatment modality for CCH.
However, CCH is typically thicker than choroidal neovascular lesions and has a distinct circulation characteristic showing an early well-defined area of intense hyperfluorescence, often followed by dye washout in late frames on indocyanine green angiography.15 The depth of vascular occlusion by PDT treatment depends on the total light dose delivered.14,16 Consequently, most studies using PDT for CCH modified standard protocol adapted in the treatment of age-related macular degeneration.14-17 These modifications included higher exposure levels, bolus dye administration, and shorter time interval between dye infusion and laser application. In addition, Porrini et al.16 reported that additional sessions of PDT were required to achieve complete regression in cases of thicker CCH. Modified PDT and multiple sessions of PDT are thought to increase the risk of over treatment effects, such as retinal ischemia or choroidal occlusion with subsequent RPE atrophy. Some cases of focal chorioretinal atrophy were reported in previous studies using a modified and intensified PDT protocol or multiple session of PDT.14,16
Ziemssen et al.25 reported a case of juxtapapillary retinal capillary hemangioma, successfully treated with a combination of intravitreal bevacizumab and PDT. The investigators believed that the anti-exudative effect of bevacizumab offers better delineation of the underlying choroidal lesion and consequently allows more precise adjustment of the PDT to minimize complications such as transient visual disturbance and chorioretinal atrophy.25 Therefore, we considered combination therapy with intravitreal bevacizumab (1.25 mg) and PDT (verteporfin 6 mg/m2 over 10 minutes, a radiant exposure of 50 J/cm2 with an exposure time of 83 seconds) in the second and third patients who had thicker CCHs. Combination therapy induced marked tumor regression and improved visual acuity resulting from disappearance of the subretinal fluid. However, the second patient had focal chorioretinal atrophy in the lesion treated with PDT. It is thought that bevacizumab decreases the tumor thickness through resorption of subretinal fluid, and this may increase the irradiation dose delivered by PDT. Thus, further studies on the optimal reduced dose of PDT are still needed to minimize PDT-associated complications in combination therapy.
In summary, intravitreal bevacizumab showed encouraging effect to increase visual acuity through inducing resorption of subretinal fluid associated with CCH. Bevacizumab therapy combined with PDT achieved marked atrophy of the tumor with reducing the necessity of further destruction by repeated and overdosed PDT. Therefore, we believe that intravitreal bevacizumab may be considered as a new treatment modality in patients with thin CCH and the combination therapy can be chosen as more effective treatment to decrease the risk of PDT-associated complications in patients with thick CCH than PDT alone.
