A Case of Myotonic Dystrophy With Pigmentary Retinal Changes
Article information
Abstract
A 46-year-old man presented with visual disturbances in both eyes. His best corrected visual acuity was 0.7 (both eyes). Ptosis and limitation of ocular movement in every direction were observed. Slit lamp examination showed a bilateral iridescent cataract. Fundus examination showed peripheral depigmentation of the retinal pigment epithelium and pigmentary clumping in both eyes that agreed with blocked fluorescence and widow defects on fluorescein angiography. The amplitude of b-wave was decreased on electroretinography. Fourteen months later, the patient's best corrected visual acuity decreased to 0.3 due to increased lens opacity. Phacoemulsification and intraocular lens implantation were performed on both eyes. At the patient's final visit, retinal findings were stable with a best corrected visual acuity of 0.7 in both eyes. In conclusion, the visual disturbance could have been caused by both cataracts and retinal degeneration, meaning the fundus should be examined carefully in patients with myotonic dystrophy.
Myotonic dystrophy is an inherited disorder accompanied by progressive wasting and weakness of the distal muscles and myotonia.1 Cases of myotonic dystrophy are generally classified as one of two types: type 1 myotonic dystrophy has amplifications of an unstable trinucleotide CTG repeat located on chromosome 19, while type 2 has CCTG expansion on chromosome 3. Recently, a new classification, proximal myotonic myopathy (PROMM), was also proposed.2
Ocular complications in myotonic dystrophy include ptosis, weakness of the ocular muscle and cataracts. Cataracts are useful for diagnosing myotonic dystrophy since they are present in nearly all patients with the condition.4 Other features of myotonic dystrophy include sluggish pupillary response, low intraocular pressure, and retinal degeneration. In Korea, cataracts associated with myotonic dystrophy have been reported,5 but retinal degeneration has not. Here, we report the first Korean case of retinal degeneration in myotonic dystrophy with literature reviews.
Case Report
A 46-year-old man was referred for ophthalmologic examination due to gradually decreasing visual acuity. He had suffered from disturbances of ocular movements, ptosis and weakness of the extremities for two years. Through polymerase chain reaction (PCR), the patient was found to have amplification of CTG repeats on chromosome 9, which is compatible with myotonic dystrophy type 1.
On ophthalmologic examination, the patient's best corrected visual acuity in both eyes was 0.7. Intraocular pressure was 13 mmHg in the right eye and 15 mmHg in the left eye. The levator function was 0 mm in the right eye and 1 mm in the left eye. In the primary position, exotropia of 10 prism diopters was found. Limitation of ocular movement was observed in every gaze direction (Fig. 1). On slit lamp examination, a bilateral iridescent cataract was noted. Fundus examination showed geographic depigmentation of the retinal pigment epithelium along the vascular arcade and pigment clumps in the peripheral area (Fig. 2A) in both eyes. Fluorescein angiography showed blocked fluorescence by pigment clumps and window defects (Fig. 2B). The b-wave amplitude was decreased on electroretinography. Eye movement recordings showed slowed saccades and impaired smooth pursuit.

Bilateral ptosis and ophthalmoplegia with exotropia in every gaze direction.
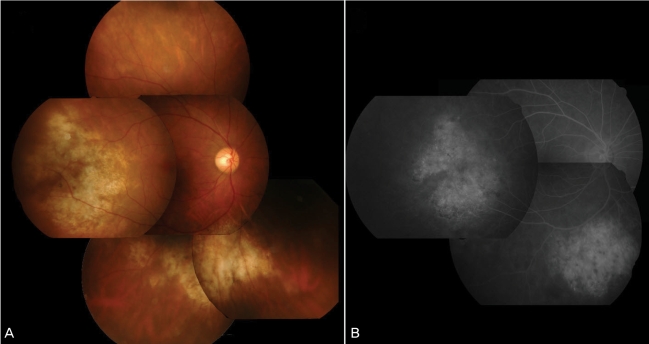
(A) A fundus photograph demonstrates peripheral geographic depigmentation of the retinal pigment epithelium and pigmentary clumpings. (B) Fluorescein angiographic examination reveals blocked fluorescence due to clumping retinal pigment epithelium and window defects.
Fourteen months later, the patient's best-corrected visual acuity had decreased to 0.3 in both eyes. Phacoemulsification and intraocular lens implantation were sequentially performed in both eyes and his best-corrected visual acuity improved to 0.7. Fundus examination showed no significant interval changes.
Discussion
Myotonic dystrophy type I is caused by a genetic defect composed of an expansion of cytosine-thymidine-guanine (CTG) repeats, resultingin a defect of the dystrophia myotonica protein kinase (DMPK) gene and a reduction of DMPK messenger RNA expression. This genetic defect affects zinc finger protein 9 expression.6
The most common ocular complications associated with myotonic dystrophy are cataracts that may be induced by a defect of the lens epithelium.7 As in the present case, they generally have the appearance of iridescent dust and fine points with colored crystals.3
Various retinal degenerations associated with myotonic dystrophy include a butterfly pattern in the macular area, peripheral reticular pigmentary changes, and polymorphic atrophy.8 Peripheral reticular pigmentary change is the most common form of retinal degeneration and was observed in the present case. This pigmentary change causes decreased b-wave amplitude on electroretinography which we also observed.3 Kimizuka et al.9 report on atrophy of the inner retinal layers with preservation of the photoreceptors in the peripheral retina and increased pigmentation with granular, striate or satellite patternin the macula.
The reduced saccadic peak velocity and impaired smooth pursuit gain in the present case were almost identical with those observed and described in a previous report.10 Lessell S et al.10 reported that limitation of ocular movement and ptosis may be due to one or all of three possible mechanisms: supranuclear control, peripheral motor apparatus and extraocular muscle atrophy. Previously reported histological findings showed pathological changes with a shredded appearance and an abundance of lipofuscin in muscle fibers.11
In conclusion, the visual disturbances associated with myotonic dystrophy may be caused not only by cataracts but also by retinal degeneration. Therefore, fundus examination is essential and should be performed carefully in patients with myotonic dystrophy.