

Endophthalmitis after intraocular surgery is rare but may be accompanied by serious complications. Among various causative agents of endophthalmitis, gram-negative bacteria is well known for its fast progression and poor prognosis.1
Sphingomonas paucimobilis is gram-negative bacillus that is widely distributed in the natural environment. It has been reported to cause opportunistic infection in immuno-compromized hosts.2 We present a case of an acute onset of delayed postoperative endophthalmitis that was caused by S. paucimobilis.
Case Report
A 62-year-old healthy man was transferred to our hospital. He had uneventful phacoemulsification and the posterior chamber intraocular lens (IOL) implantation in the right eye in a private clinic 3 months ago. Review on the first postoperative day, and follow-up was unremarkable and no procedure such as suture removal or YAG capsulotomy was done. His medical history was not significant, and a review of systems failed to indicate any potential signs or symptoms of chronic or malignant disease. He experienced sudden ocular pain and the deterioration of visual acuity the day before his visit. At a private clinic, he received intravitreal vancomycin (1 mg/0.1 ml) and amikacin (0.4 mg/0.1 ml) but. the condition became worse. He was transferred to our hospital with a sample of vitreous humor obtained during the intravitreal injection.
At the time of transfer, examination revealed visual acuity of hand motion in the right eye and 20/25 in the left eye. The intraocular pressure (IOP) was 28 mmHg in the right eye and 14 mmHg in the left eye. The right eye was intensely injected; 4+ cells in the anterior chamber, 2 mm hypopyon, mid dilated-fixed pupil, grade 4 vitreous opacity and a very weak red reflex degree were noted on examination (Fig. 1A). B-scan ultrasonography showed floating materials in vitreous. The WBC count was 14100/mm3, and C-reactive protein (CRP) value was positive at 92.2 mg/dl. The chest X-ray and ultrasound scan of abdomen and heart showed no abnormalities.
On that day, we aspirated some vitreous humor and sent it to the laboratory for Gram's staining. In the Gram's staining, gram-negative bacilli were detected. We performed pars plana vitrectomy using 175 µg/ml ceftazidime in the irrigating solution,3 IOL explantation, removal of the capsular bag and intravitreal ceftazidime (2.25 mg/0.1 ml) injection. During the vitrectomy, we saw severe cyclic membrane and thick exudative membrane that covered the entire retina. After delicate vitrectomy like shaving, we could see the disc and major vessel arcade faintly. The vitreous humor obtained during vitrectomy and the IOL were sent to the laboratory for smear and culture test.
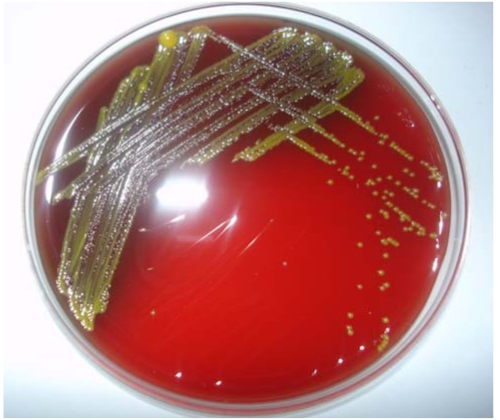
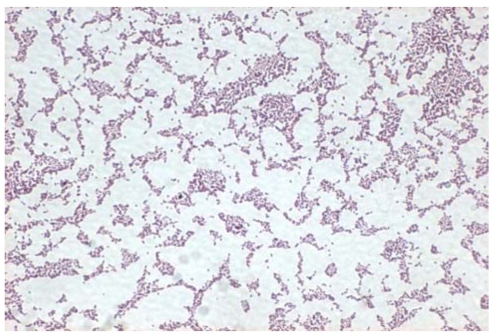
The day after the vitrectomy, severe stromal edema in cornea and mild fibrous membrane at the pupil were detected. The patient received ceftazidime 1 g (2 times/day) and tobramycin 80 mg (2 times/day) intravenously. He was treated with fortified ceftazidime (50 mg/ml) and levofloxacin eyedrops every 30 minutes and oral prednisolone 45 mg daily. Two days postoperatively, in the culture of aspirated vitreous during vitrectomy and the vitreous humor from the private clinic, the same bacteria Sphingomonas paucimobilis was isolated (Fig. 2 and 3). Disk susceptibility on Mueller-Hintom agar demonstrated susceptibility to ampicillin, aztreonam, cefoperazone, ceftazidime, gentamicin, imipenem, and peperacillin and resistance to tobramycin.
Two weeks postoperatively, the IOP in the right eye was 12 mmHg. 1+ cells in the anterior chamber, the reduction of the exudates in the peripheral retina, and grade 1 vitreous opacity were detected. Three months postoperatively, the best corrected visual acuity improved to 20/300. No cells were found in the anterior chamber or vitreous cavity. A mild pale color of optic disc and macular degeneration like pigmentary changes were detected (Fig. 1B).
Discussion
Infectious endophthalmitis generally refers to the inflammatory condition in the eye due to bacterial infection or fungal infection. Among the pathogens of infectious endophthalmitis occurring after cataract surgery, gram-negative bacteria have been reported in 6% and its prognosis is known to be worse than gram-positive bacteria.1
Sphingomonas paucimobilis (formerly categorized as CDC group IIK, biotype 1) is an aerobic, nonfermenting, oxidase and catalase positive, gram-negative bacillus. Among gram-negative bacteria, Pseudomonas aeruginosa are highly toxic, but nonfermentative bacillus has low toxicity and thus they are known to be clinically unimportant bacteria. In 1990, its designation was changed from genus pseudomonas to genus sphingomonas that is used until now.4
Since 1979 when S. paucimobilis infection was reported in human for the first time, it has been reported primarily in the immuno-compromized patients with the long-term insertion of the central venous catheter as the opportunistic infection pattern such as peritonitis, meningitis, septicemia, etc.2 Clinically, S. paucimobilis seems to be of only limited pathogenic potential. This may be explained by the lack of lipopolysaccharide A, which is replaced by glycosphingolipid Gas the major structural component of its gram-negative cell wall.5 Studies have shown that glycosphingolipid is 105-fold less active than lipopolysaccharide A when inducing the release of tumor necrosis factor-α, interleukin-6, and interleukin-1 by mononuclear cells.6 The absence of lipopolysaccaride in the cell wall of S. paucimobilis may explain the relatively favorable clinical course of postoperative endophthalmitis in our patient as would have been expected from lipopolysaccharid-containing gram-negative bacillus.
S. paucimobilis has been reported to be sensitive to aminoglycoside (either alone or in combination with a β-lactam antibiotic) or quinolone. Other report showed variable antibiotic susceptibility.7 Therefore, the treatment should be guided by antibiotic susceptibility studies. We got the result of the Gram's staining before the vitrectomy. So we used ceftazidime in vitrectomy as the broad spectrum antibiotic to cover the gram-negative bacilli. Fortunately, there was ceftazidime in the result of disc susceptibility test.
To date, there has been only one reported case of endophthalmitis caused by S. paucimobilis.8 It was a case of recurrent acute endophthalmitis with complete resolution only after vitrectomy and this organism was resistant to initial medical treatment. In our case, diagnosis and treatment by vitrectomy were performed immediately after onset endophthalmitis. And in common with a previous report, the source of this bacteria causing postoperative endophthalmitis remains uncertain.
Endophthalmitis caused by S. paucimobilis can be developed as the acute onset of delayed type. Our patient was a healthy man without systemic disease.
He had an uneventful cataract surgery and visual acuity was very good postoperatively. We performed vitrectomy using ceftazidime in the irrigating solution, complete removal of the capsular bag, IOL, and inflammatory membrane on the ciliary body and vitreous cortex. At the same time, we injected ceftazidime intravitreally. In both vitreous humor obtained during vitrectomy and from a local clinic, the same S. paucimobilis was isolated and thus the diagnosis of endophthalmitis by S. paucimobilis was confirmed. The result of susceptibility tests reported ceftazidime that we had used in vitrectomy. We think these procedures have contributed to the favorable result.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






