Suture Fixation Technique for a Single-piece Foldable Closed-loop Intraocular Lens
Article information
Abstract
Purpose
We describe a suture fixation technique for a single-piece foldable acrylic closed-loop intraocular lens (IOL) (C-flex™, Rayner).
Methods
In our experimental model analyzing the stability of acrylic haptics, we confirmed that the IOL could be in counterpoise without tilt using only a two-point fixation. This new surgical technique was performed in seven patients.
Results
The unique haptic design allows easy and secure suture fixation. The clinical outcomes were encouraging.
Conclusions
It is conceivable that better stabilization can be achieved by the broad arc of distal haptic-tissue contact, in addition to suture fixation, using our surgical technique with the C-flex™ IOL.
The eyelets on the polymethyl methacrylate (PMMA) intraocular lens (IOL) haptics permit sutures to be placed easily at symmetrical points. Various four-point fixation techniques using the eyelets have been shown to yield better stability and prevent tilt.1-5 Suture fixation of PMMA IOLs requires at least 6.0 mm incisions, so many authors have recently used foldable IOLs for suture fixation through a small incision.6-8 However, foldable IOLs are manufactured in a form that has no eyelets on the haptics. Thus, tying the sutures at symmetrical haptic points can be technically difficult. Tilt, decentration, and inadvertent slippage of the sutures have all been considered as possible complications.
We speculated that a closed-loop design of a Rayner single-piece acrylic IOL (C-flex™) could serve the function of eyelets. However, it has not yet been determined if suture fixation using the acrylic haptics results in stability of the IOL, which is very flexible. In this study, we conducted a simple experiment to clarify this issue with regard to patient application.
Materials and Methods
Experiment
We designed an experimental model using Vernier calipers in which a cylindrical bar with a groove approximately 0.3 mm in depth was attached perpendicular to the outward gauge tip to prevent slippage of the sutures. A blue IOL was used for better contrast with the background.
Based on reports regarding the mean diameter of the ciliary sulcus,9,10 the scale of the Vernier calipers was adjusted to 11.0 mm. We selected point A and point B on the IOL as suture placement sites (Fig. 1). Point A is a classical suture placement site because it is on the longest diameter of the haptic spread (12 mm). We used Point B as a novel suture placement site for this study because the tapered configuration presented an ideal location for attaching the suture. The diameter of the haptic spread at point B was 10 mm. A 10-0 polypropylene (Prolene®) suture was placed at either point A or point B on each haptic, and the free ends of the sutures were fixed to the cylindrical bar. The IOL behaved differently because of a difference in the distances between the cylindrical bars and the suture fixation sites. In cases with placement of the suture at point A, the outer haptics were slightly compressed inward. In contrast, in cases with placement of the suture at point B, the outer haptics were separated from the bar. However, the IOL could be fixed in a counterpoise without significant tilt in both cases without reference to the haptic-bar contact (Fig. 2). We hypothesized that a broad-based (3 mm) haptic design could maximize the stability of the haptic-optic junction. Suture fixation of the C-flex™ IOL was performed after informed consent was obtained from the seven patients in the study.
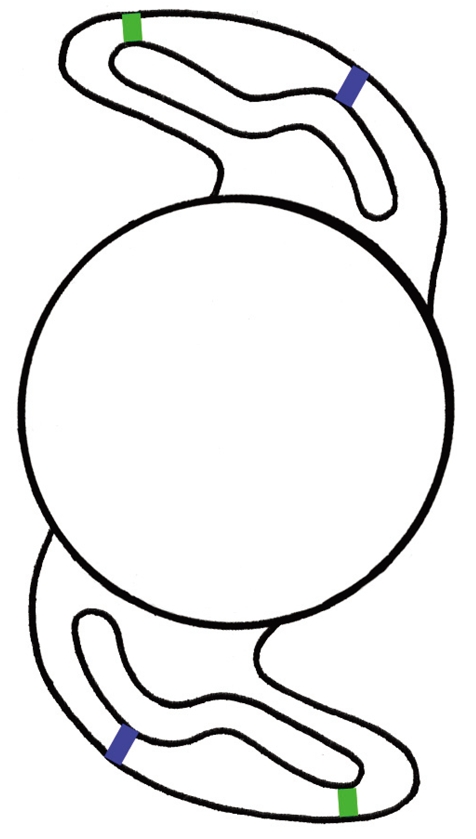
Schematic drawing of a C-flex™ IOL with wide haptic-optic junctions (3 mm in length). Point A is colored in green and point B is colored in blue.
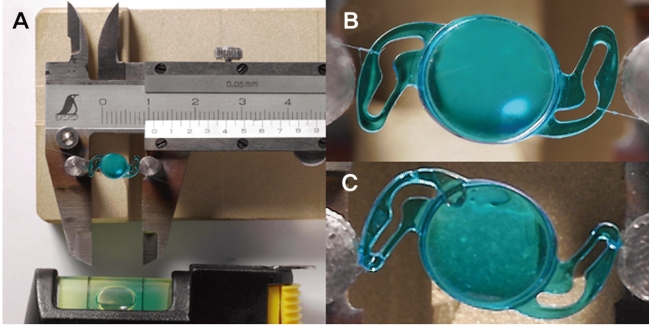
Suture fixation of a C-flex™ IOL in our experimental model. (A) Each step was carried out in a horizontal plane using a level. (B) and (C) Close-up photographs after suture fixation.
Surgical technique
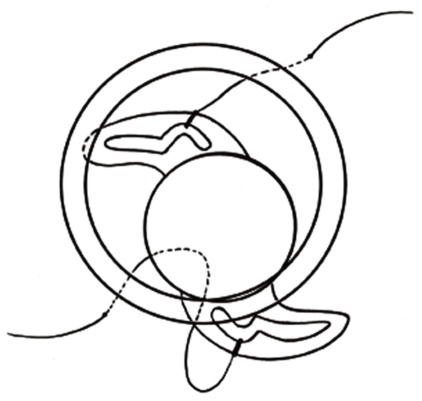
All surgeries were performed by a single surgeon. Two fornix-based conjunctival peritomies were made 180 degrees apart (usually from 2 to 4 o'clock and from 8 to 10 o'clock) followed by the construction of 3×3 mm partial thickness triangular limbus-based scleral flaps. One arm of a double-armed 10-0 Prolene (Ethicon, STC6) suture on a long straight needle was passed 1 mm posterior to the limb ab externo underneath the scleral flap and docked into a 26-gauge needle inserted in a similar fashion from the opposite side. The 26-gauge needle with the 10-0 Prolene suture was then withdrawn, resulting in the 10-0 Prolene suture bridging the posterior chamber. The suture was then externalized through a 3.0 mm beveled corneal incision (12 o'clock position) using a Sinskey hook and cut. Before placing the IOL in the injector, one end of the 10-0 Prolene suture was threaded through the injector and tied at point A on the leading haptic. The IOL was then loaded into the injector and the leading haptic was inserted into the posterior chamber (Fig. 3).

One free end of the suture is passed from the 8 o'clock position through the insertion tip of the injector and tied to the leading haptic. The IOL is loaded into the injector after the suture is pulled out with forceps and tied at the leading haptic.
It was not necessary to extend the corneal incision because the diameter of the insertion tip was only 2 mm. The trailing haptic was purposefully left outside the eye and secured with the other end of the 10-0 Prolene suture before insertion into the posterior chamber (Fig. 4). Tension was adjusted as necessary to center the IOL. The needle of each arm of the suture was passed through the scleral bed underneath the flap to form a loop. The needle was then cut off and the suture end was firmly tied to the loop. The scleral flap was then securely repositioned with a single 10-0 nylon suture.
The other free end of the suture is passed from the 2 o'clock position and tied to the trailing haptic outside the eye.
Results
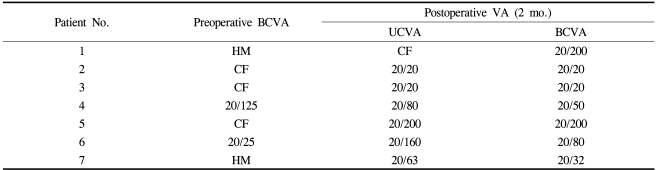
Three of the seven patients underwent this procedure in combination with a pars plana vitrectomy, one of whom underwent this procedure in combination with both a pars plana vitrectomy and an intravitreal gas injection (Table 1). Sufficient anterior vitrectomies were performed in the other four patients, and residual lens capsules and anterior vitreous in the pupil area were removed. The postoperative course was uneventful, and slit-lamp examination showed stable placement of the IOLs without tilt or decentration in six patients (Fig. 5A). One eye (patient 4 in Table 1) had an IOL that was slightly decentered in an inferior direction (Fig. 5B). The UCVA at 2 months after surgery was 20/20 in three patients, and had improved significantly at 1 month after surgery in all seven patients. Visual recovery was limited in three patients with underlying vitreoretinal diseases.
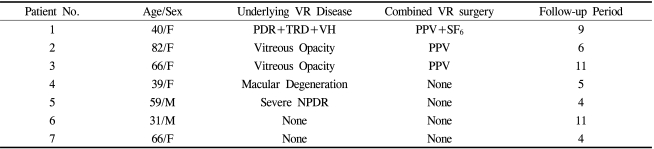
Clinical Characteristics of Patients (N=7)
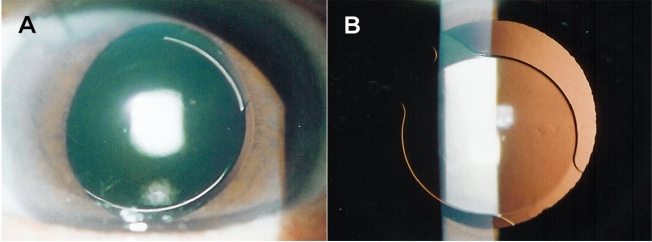
Slit-lamp examination at 1 week after surgery. (A) A well-centered IOL. (B) An IOL slightly decentered in an inferior direction.
There were no significant complications such as vitreous or choroidal hemorrhage, retinal detachment, or endophthalmitis during the follow-up period.
Discussion
Three-piece foldable IOLs have been used for suture fixation through a small incision because PMMA haptics confer mechanical stability.6-8 Suture fixation of a single-piece acrylic IOL was reported in a child with severe bilateral ectopia lentis.11 It was inferred that increased flexibility at the acrylic haptic-optic junction of the IOL could possibly result in optic tilt, despite stable positioning of the haptics in the ciliary sulcus. Optic tilt did not occur in our experimental model using the C-flex™ IOL, suggesting that a wide haptic-optic junction may prevent distortion of the IOL.
In suture fixation of IOLs without eyelets on the haptics, the point of maximum haptic spread has been used to accurately place sutures.6,12 The haptics should compress the tissue in the long arc to improve IOL stability because their fixed area is equal to the contact area in the ciliary sulcus. Consequently, IOLs≥13.0 mm in overall diameter are used most frequently. However, it has been reported that the distal portion of the haptics may lie on the pars plitica and pars plana, rather than fitting in the ciliary sulcus, when the sutures are tied to haptics near the optic center.12 The reason for this result is that long and rigid PMMA haptics may compress the tissue, the IOL may be tilted, and eventually the distal portion of the haptics may be displaced in a posterior direction. Also, suture slippage may develop due to the open-loop haptic design. However, in the case of the C-flex™ IOL, the relatively small diameter of the IOL (12 mm) and its flexibility should not cause excessively strong tissue compression, resulting in total ciliary sulcus fixation of the haptic. The tapered configuration at specific locations of the haptic provided an easily reproducible, secure, and symmetrical landmark for suture fixation and prevented suture slippage.
In all cases, point B of the haptic was selected as a suture placement site. It is impossible to achieve haptic-tissue contact due to the short diameter of the haptic spread (10 mm) at point B. However, the diameter of the haptic spread increases gradually toward the distal portion of the haptic, and the diameter of the haptic spread at point A (12 mm) exceeds the mean diameter (11 mm) of the ciliary sulcus. Consequently, a portion close to the ends of the haptics contacts the tissue in a broad arc, this presumably results in increased stability of the IOL (Fig. 6).
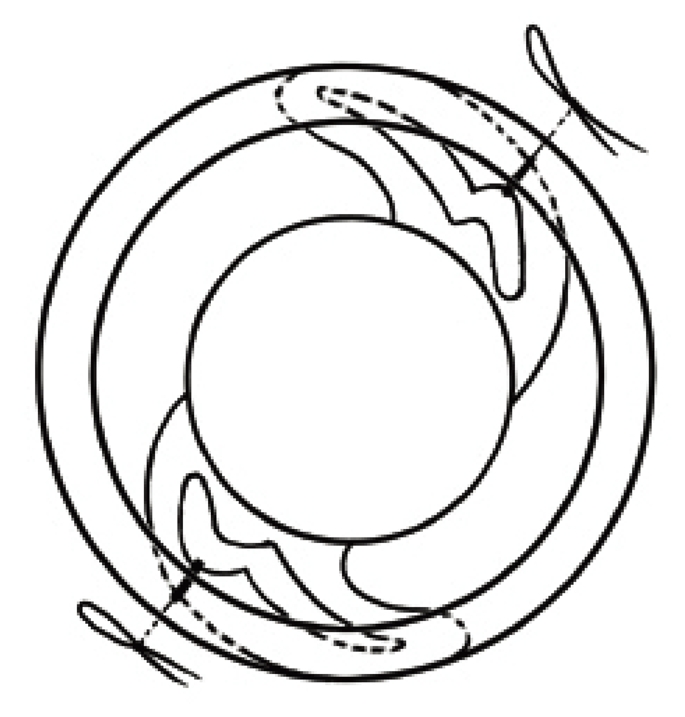
The broad arc of distal haptic-tissue contact in the two-point suture fixation technique.
Kuckle et al13 reported histopathological evidence of sulcus scarring of both haptics in a scleral-fixed IOL. In this regard, the broad arc of distal haptic-tissue contact is surrounded by a fibrous capsule, which results in the IOL firmly adhering to the tissue over time. Therefore, it is believed that, in addition to two-point fixation, another distal haptic-tissue adherence could provide resistance to torsional forces and better stability, similar to the four-point fixation technique.
The incidence of vitreous hemorrhage is increased in the previously described four-point fixation technique, in which four scleral punctures are required. However, IOL stability can be achieved immediately following surgery.14 In contrast, our technique requires only two scleral punctures with a small incision, resulting in a significantly lower incidence of vitreous hemorrhage.
Taskapili et al15 performed suture fixation in 20 eyes with a single-piece acrylic IOL similar to the C-flex™ IOL. However, in contrast to our surgical technique, they selected a distal point of the haptic for suture fixation and used forceps to insert the IOLs. Since our technique uses an injector system instead of folding forceps to insert the IOLs, entanglement of the stitch in the folding forceps can be avoided.6-8,11
However, some considerations should be given to suture fixation of the C-flex™ IOL. First, it is technically difficult to produce a wide haptic-tissue contact area because of the relatively shorter overall diameter of the IOL in patients with severe myopia. In these patients, IOLs with longer haptic spreads are recommended. In this study, one patient with severe myopia (axial length: 30.05 mm) had postoperative decentration, probably due to a short haptic spread compared to the diameter of the ciliary sulcus. Second, chronic inflammation can be induced by rubbing between the iris and the IOL optic since the C-flex™ IOL has no haptic angulation. However, a previous study reported that contact between the iris and the IOL optic was observed in IOLs with haptic angulations ranging from 5 to 10 degrees, even when the IOLs were properly sutured at the ciliary sulcus.16 In this study, no significant postoperative inflammation was observed in any of the patients. Third, postoperative IOL tilting was not objectively measured. However, slit-lamp examination showed central placement of the IOL without clinically evident tilting, even in the one eye which underwent vitrectomy and gas tamponade.
In summary, the closed-loop design of the C-flex™ IOL allows easy and secure suture fixation, even in vitrectomized eyes. In addition, we believe that our fixation technique using the unique haptic design of the C-flex™ IOL has clinical outcomes similar to those of the four-point fixation technique. However, further studies with a larger number of cases and a longer follow-up period are needed to evaluate the safety and effectiveness of our suture fixation technique.