Ciliary Sulcus Ahmed Valve Implantation
Article information
Abstract
Purpose
Ahmed glaucoma valves were implanted into the ciliary sulcus of two patients diagnosed with neovascular glaucoma with favorable outcomes.
Methods
The study patients presented to our hospital with ocular pain caused by increased intraocular pressure (IOP). A thorough history was taken, and an ophthalmic examination was performed.
Results
A 71-year-old male patient and a 57-year-old female patient visited our hospital for ocular pain and persistent, elevated IOP. Each were diagnosed with neovascular glaucoma and underwent an Ahmed glaucoma valve implantation to the sulcus. After surgery, the patients maintained stable IOPs without major complications.
Conclusions
The method of Ahmed glaucoma valve implantation into the ciliary sulcus could reduce complications caused by implantation to the anterior chamber. It is thought to be an efficient method for the maintenance of appropriate IOP after surgery.
Ischemia in the posterior segment of eye can occur in patients with neovascular glaucoma, and diverse therapeutic methods have been developed to combat this problem.1,2 It is known that by performing panretinal photocoagulation first, the synthesis of factors that induce new blood vessel growth in the posterior segment of eye is suppressed, and migration of these factors to the anterior segment of the eye is thus prevented, allowing for the regression of new blood vessels. The success rate of trabeculectomy and other general glaucoma surgeries varies widely, from approximately 10 to 78%. Nonetheless, for neovascular glaucoma, the tendency to bleed is high, and therefore the success rate has been reported generally to be poor.3-6
For refractory glaucoma patients with a poor surgical prognosis, implants have been widely used, particularly the recently developed Ahmed glaucoma valve implant (New World Medical, Inc. Rancho Cucamonga, California, USA), which has been reported to reduce the initial hypotony after surgery, among other related complications.7-9
We implanted Ahmed glaucoma valves (New World Medical, Inc. Rancho Cucamonga, California, Model FP7) in the sulcus of two patients diagnosed with neovascular glaucoma. We were able to obtain satisfactory intraocular pressures (IOP) without major surgical complications. Since this method that has not been yet been reported in the literature, the cases are reported here with a review of the literature.
Case
Case 1.
A 71-year-old male with diabetes mellitus presented to our hospital with a chief complaint of left ocular pain that progressively worsened over the course of three months. One year ago, he underwent bilateral cataract extraction with intraocular lens (IOL) implantation. The patient had also been experiencing visual disturbances and had been treated with eye drops prior to transfer to our hospital.
At the initial examination, the best corrected visual acuity of the right eye was 0.7, and the best corrected visual acuity of the left eye was 0.3. The IOP of the right eye measured by Goldmann applanation tonometry was 12 mmHg, and the left eye was 34 mmHg. On slit lamp examination of the left eye, new blood vessels on the iris surface and adhesion of the new blood vessels to the adjacent peripheral anterior synechiae were detected. Panretinal photocoagulation was performed on the left eye, and topical steroids and atropine, were administered. For IOP control, a topical beta-blocker (Calte®, Hanlim Pharm Co., Korea) and an oral carbonic anhydrase inhibitor (Mezomin®, Keukdong Pharm Co, Korea) were administered. Nevertheless, the IOP of the left eye measured by the Goldmann applanation tonometry was 40 mmHg. Hence, an Ahmed glaucoma valve implantation was performed.
The implantation was performed under retrobulbar anesthesia. In the middle of the superior rectus muscle and the lateral rectus muscle, the fornix conjunctiva was incised approximately 8 mm from the limbus. The conjunctiva and the tenon's capsule were dissected from the sclera, and a limbal-based scleral flap 4×4 mm in size was prepared. The Ahmed glaucoma valve was implanted to the site between the superior rectus muscle and the lateral rectus muscle and fixed to the sclera with 10-0 nylon. Prior to the implantation of the Ahmed glaucoma valve, a 1 cc balanced salt solution (BSS®, Alcon, USA) was administered through the Ahmed glaucoma valve using a 26 G cannula in order to confirm correct functioning. Approximately 2 mm of the silicon tube was implanted on the inside of the posterior chamber, and the end of tube was cut at 30° degrees. Using a 23 G needle, the posterior chamber was perforated through the sulcus, and the tube was implanted (Figure 1). We confirmed that the tube was implanted in the correct position through dilated pupil. The area of the exposed tube was covered with the scleral flap and fixed to the sclera with 10-0 nylon, and the tenon's capsule and the conjunctiva were sutured with 10-0 nylon. One week after surgery, the left eye visual acuity was 0.04, the IOP was 5 mmHg, and on examination of the fundus, choroidal detachment was observed. Nonetheless, visual acuity two weeks after surgery improved to 0.08. The IOP was 8 mmHg, and on examination of the fundus, choroidal detachment was improved. One month after surgery, visual acuity was 0.4 and IOP had increased to 26 mmHg; consequently, a topical carbonic anhydrase inhibitor (Cosopt®, MSD, USA) was administered. Two months after surgery, visual acuity improved to 0.5, with a stable IOP of 17 mmHg. On slit lamp examination, regression of new vessels in the iris surface was seen.
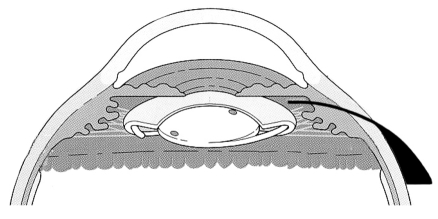
The tube is inserted through the ciliary sulcus.
Case 2.
A 58-year-old female presented to our hospital with a four month history of right ocular pain that had progressively worsened. Two years prior, she underwent cataract extraction with IOL implantation, and during the first year postoperatively, she received panretinal photocoagulation therapy. One year ago, she underwent a pars plana vitrectomy for proliferative diabetic retinopathy. The patient was diagnosed with diabetes 17 years ago, but otherwise did not have a significant past medical history.
At the initial examination, the best corrected visual acuity of the right eye was 0.08, and the left eye was 0.3. The IOP of the right eye was measured using the Goldmann applanation tonometry and was 35 mmHg; the left eye was 14 mmHg. On slit lamp examination, new vessels on the iris surface were detected, and in the anterior chamber angle examination, new vessels had formed. Due to the continuous proliferation of the fibrovascular membrane, closure of the right anterior chamber angle was detected. Topical beta-blockers and topical carbonic anhydrase inhibitors (Cosopt®, MSD, USA) were continuously administered, and photocoagulation for new vessels in the anterior chamber was performed. However, the ocular pressure could not be controlled; hence, an Ahmed glaucoma valve implantation was performed.
Surgery was performed by the method identical to the Case 1. In this case, however, due to the small size of her pupil, we examined the location of tube by using a Hirschman iris hook (Bausch & Lomb, Inc. St. Louis, Missouri). Four months after surgery, a slightly elevated IOP level at 20-22 mmHg was maintained. Five months after surgery, the visual acuity of the right eye was 0.08, and the IOP of the right eye stabilized to 17 mmHg. On slit lamp examination, the result of the regression of new vessels in the iris surface was detected (Fig. 2). Ten months after surgery, during the patient's final visit to our outpatient clinic, her visual acuity had not improved, but she did not have hypotony, hyphema, choroidal detachment or other complications, and her IOP was well-maintained at 12-17 mmHg.
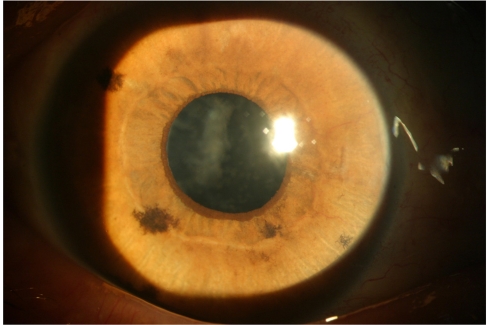
Postoperative finding show regression of iris neovascularization.
Discussion
Neovascular glaucoma is a disease in which new vessels are formed in the iris due to the ischemia of the posterior segment of eye. The new vessels cause the occlusion of the trabecular meshwork resulting in the elevation of IOP in patient with diabetic retinopathy, branched retinal vein occlusion, carotid artery disease, etc. IOP cannot be controlled readily by medical treatments, and the risk of hemorrhage with the conventional filtering surgery for glaucoma trabeculectomy is high. The anterior chamber is occluded due to the continuous proliferation of the fibrovascular membrane. The surgery's success rate is low because of excessive wound healing reaction.3
In order to avoid these complications, the frequency of glaucoma drainage device implantation is on the rise. After first designed by Zorab,10 glaucoma drainage devices have continuously improved in terms of concept, materials, and shapes. The Ahmed drainage device used in our experiment has a unilateral valve to prevent hypotony. Theoretically, the valve is open at the pressure between 8-10 mmHg, and in cases where the IOP is lower than that, the valve is closed and controls the flow of the aqueous humor. Therefore, the Ahmed drainage device is designed to prevent postsurgical hypotony.7 The device used in our cases has a silicone body with a connected silicone tube. The inner diameter of the silicone tube was 0.305 mm, the outer diameter was 0.635 mm, the surface area of the silicone body was 184 mm2, the length was 16 mm, the width was 13 mm, and the thickness was 0.9 mm. The valve system used to prevent hypotony consisted of a thin silicone elastomer membrane.
The complications reported after the Ahmed glaucoma valve implantation are hypotony, anterior chamber collapse, choroidal detachment, hyphema, tube malposition, tube occlusion, and extraocular movement (EOM) limitation, etc. Kim et al11 have reported that they performed Ahmed glaucoma valve implantation for six years, and in 114 eyes of 112 patients who were available for postoperative follow-up for at least six months. The patients' clinical course was examined and complications were noted. It was found that hyphema occurred in 14% of patients, which was the most prevalent complication. In addition, there was also choroidal detachment, development of a shallow anterior chamber caused by hypotony, tube occlusion, tube malposition, endophthalmitis, as well as other complications.
In the cases where the Ahmed glaucoma valve was implanted in the anterior chamber, and in the cases involving peripheral anterior synechiae in the adjacent iris, iris dialysis can develop. In cases where the tube is malpositioned, the tip of the glaucoma valve may contact the cornea, which may induce corneal decompensation.11-14 Hu et al14 claimed that during the valve implantation perforation with a needle parallel to the iris is important while performing anterior chamber paracentesis. There are several reasons causing corneal decompensation. Corneal decompensation occurs when the aqueous humor of the corneal area located near the tube affects corneal endothelial cells. This can occur in cases when a patient rubs his/her eyes or blinks his/her eyes intensely, when technical damage caused by tube-cornea contingence, inflammation cause by tube-iris contingence, or because of a chronic foreign body reaction to the tube.15,16
Methods of Ahmed glaucoma valve implantation can be classified according to the location of the drainage device tube, to implant the device in the anterior chamber or to implant the device into the vitreous; the former may induce tube malposition, iris injury, and anterior chamber angle injury, and the latter may reduce the injury in the cornea, the iris, and the anterior chamber angle. Also the shortcomings of the latter are that the procedure is useful only for the eyes that underwent a previous vitrectomy, and even so, the base of the vitreous must have been removed thoroughly.
Recently, an Ahmed glaucoma valve for implantation in the vitreous (Pars plana clip™) was also developed and used. The former is better known in most cases, but some studies involving the latter have been reported. Regarding implantation of the glaucoma drainage devices to the vitreous, Schlote et al17 have reported that it was performed in nine patients (11 eyes), and that the success rate reached 91% one year after surgery. In Korea, Kook et al18 reported that in a refractory glaucoma patient, the combination of pars plana vitrectomy and the Ahmed glaucoma valve implantation can stabilize the IOP postoperatively.
In our cases, instead of the implantation to the anterior chamber, the drainage device was implanted to the posterior chamber through the sulcus, in two eyes, and favorable results with appropriate postsurgical IOPs were obtained. In one eye, because of initial hypotony, choroidal detachment developed, but it improved without special treatments.
The concern regarding the method of the implantation of the Ahmed glaucoma valve in the anterior chamber is that it may induce corneal decompensation due to postsurgical tube malposition as well as induce iris injury. In addition, injury of the anterior chamber angle may result in hyphema. The method of implantation to the vitreous may reduce the injury to the cornea, the iris, and the anterior chamber angle; however, it can be performed only on the eyes that underwent vitrectomy previously, and the tube tip could be occluded by the vitreous unless the vitreous base has been removed completely. The advantage of the method of implantation of the Ahmed glaucoma valve to the posterior chamber through the sulcus as used in our cases are that it does not injure the cornea, the iris or the anterior chamber angle, and it can be performed even on eyes without previous vitrectomy. Especially, it is more useful for corneal transplanted eyes and when there are small number of corneal endothelial cells.
However, it is difficult to assess the location of the tube during surgery, and the fact that the surgery could be performed on only pseudophakia or aphakia may be a shortcoming. In addition, due to the friction of the valve tube and the iris, iris pigment dispersion may develop. In one of our cases, even though pupil dilation was induced, the location of the tube could not be assessed. We confirmed the above results by using a Hirschman iris hook during surgery. It is thought that the location of the tube after surgery may be assessed more readily with the use of the the UBM (Ultrasound biomicroscopy), Carrillo et al19 detected valve tube obstruction by using UBM on a patient who was experiencing high IOP for two weeks after the Ahmed glaucoma valve implantation. Research regarding the differences of corneal endothelial cells via Specular microscopy when the Ahmed glaucoma valve is inserted in the anterior chamber versus when it was inserted in the ciliary sulcus should be performed in the future.
In our cases, two eyes received Ahmed glaucoma valve implantation in the ciliary sulcus and demonstrated a favorable outcome without major complications.
Notes
* A summary of this paper was presented as a poster at the 96th Autumn Meeting of Korean Ophthalmological Society, November 2006, Goyang, Korea