

Overaction of the inferior oblique muscle (IOOA) results in excessive elevation of eyeball in intended adduction. It is classified as primary IOOA, which is frequently shown in infantile esotropia, and secondary IOOA following superior oblique muscle palsy (SOP). Surgical corrections of IOOA includes myectomy,1 tenotomy,2,3 extirpation & denervation, 4,5 recession6-8 and anteriorization of inferior oblique muscle (IOAT).9,10
Scott first presented IOAT, which converts the vector of IO action from elevation to depression by attaching the IO anterior to the equator. IOAT is known to be effective for correction of IOOA accompanied by dissociated vertical deviation (DVD) or SOP.10,11
Kushner12 described that IOAT changes the force vector of the IO from elevation to antielevation and causes restrictive (antielevation) syndrome with restriction of elevation on abduction. Kushner12 and Mims13 reported antielevation syndrome after performing bilateral IOAT. Stein and Ellis14 said that unilateral IO weakening procedure often lead to unmasking of IOOA in the contralateral eye according to Hering's law, and that this phenomenon appeared most characteristically after IOAT. Accordingly, symmetric bilateral IOAT is recommended in many cases.
This study reports the characteristics of patients who developed antielevation syndrome after unilateral IOAT.
Materials and Methods
This study includes 8 patients with ipsilateral restriction of elevation on abduction after unilateral IOAT and more than +2 IOOA of the contralateral eye. Four patients were referred from other hospitals and 4 patients were from 24 patients who had undergone unilateral IOAT at Korea University Hospital (our hospital) from 1994 to 2003. Medical records were retrospectively reviewed.
Patients with a past history of cyclovertical muscle operation other than the IO muscle, mechanical limitation of the muscle, and disorders of the central nervous system were excluded. Visual acuity, alternate prism cover and uncover test, head tilt test, version and duction, forced duction test, initial diagnosis, the types of previous operations, and the time to develop contralateral IOOA after IOAT were analyzed. Limitation of elevation on abduction and IOOA were subjectively graded from -4 to +4 by one examiner (YAC).
Surgical corrections including IO recession of the operated eye, IOAT, or IO myectomy of the non-operated eye were carried out in 7 patients except one patient with loss of follow-up. Postoperative findings were assessed at a minimum of 6 months (12-78 months) after surgery.
In the IOAT method at our hospital, only the anterior 1/3 of the detached insertional part of the IO was attached to the lateral end of the scleral insertion of the inferior rectus muscle (IR), releasing the lateral 2/3 of the IO temporally and posteriorly without any scleral attachment (anterior 1/3 IOAT).15
Results
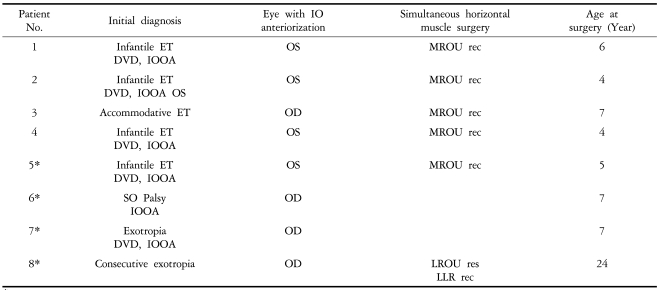
The 4 patients from our hospital included 3 patients with infantile esotropia and 1 patient with partially accommodative esotropia. They underwent unilateral anterior 1/3 IOAT for IOOA and DVD. Another 4 patients referred from other hospitals had infantile esotropia with DVD, unilateral SOP, exotropia, and consecutive exotropia, respectively (Table 1). It was found that the whole width of the IO was attached to the lateral edge of the IR insertion in these 4 patients at the time of reoperation (Table 1).
In the primary gaze, the average amount of hyperdeviation was 18.1Âą6.9 (8~30) prism diopters (PD) and limitation of elevation on abduction in eyes with IOAT was -1.5Âą1.0 (-1~-4). The degree of IOOA on adduction of the contralateral eye was +2.5Âą0.5 (+1~+4). In the 4 patients from our hospital, IOOA more than +2 of the contralateral eye followed IOAT of the other eye after 19.5Âą17.3 (4~41) months on average. The duration was impossible to calculate in the 4 patients referred from other hospitals because precise history was not known.
IOAT was performed in the contralateral eye with IOOA to produce a symmetrical IOAT status in both eyes of 3 patients from our hospital, including case 1 (Fig. 1). One patient was lost to follow-up after IOAT. Of the 4 referred patients, 2 patients underwent 14 mm recession of the anteriorized IO. One patient who had undergone IOAT of the left eye and 10 mm recession of the IO in the right eye showed severe limitation of elevation of the left eye in abduction and IOOA of the right eye. The operative finding revealed that only the anterior half of the IO fiber of the right eye was recessed by 10 mm, and the posterior half of the fiber was well preserved in the original course with intact scleral insertion behind the lateral rectus muscle (LR). This caused antielevation syndrome (Case 2, Fig. 2).
After surgical correction, the mean amount of hyperdeviation in the primary position was -1.6Âą7.7 (-10~+10) PD and the mean limitation of elevation in abduction was +0.07Âą0.6 (-0.5~-1). IOOA of the contralateral eye was +0.21Âą0.8 (-0.5~+1.5) on average (Table 2). Versional comitancy in upgazes was obtained in all patients.
1. Case 1
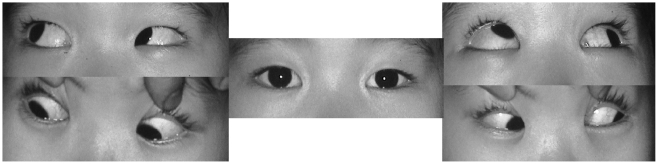
A female patient (Table 1, patient No. 2) underwent bilateral medial rectus (MR) recession and bilateral LR resection for infantile esotropia at 18 months of age. She was aligned in 5 PD esotropia, however, 5 PD hyperphoria and +3 IOOA in the left eye were observed 7 months later. IOAT was performed in the left eye at 31 months of age. Twenty months after unilateral IOAT, 12 PD hyperphoria and +3 IOOA developed in the right eye with -1 limitation of elevation on abduction in the left eye (Fig. 1-1).
At the time of reoperation, although forced duction test (FDT) revealed slight resistance in temporal-upward direction in the left eye, prominent adhesion between the previously anteriorized IO and the surrounding tissues was not found. Anterior 1/3 IO anteriorization was performed in the right eye under the diagnosis of antielevation syndrome. Six months later, IOOA in the right eye disappeared. The patient showed orthophoria in the primary gaze and almost symmetrical versional movement in upgazes despite mild upward limitation of the left eye (Fig. 1-2).
2. Case 2
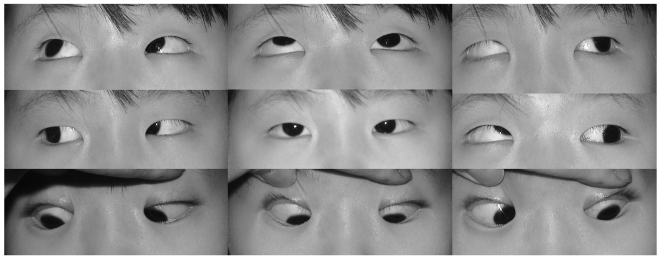
A 4-year-old female child (Table 1, patient No. 5) had a history of bilateral MR recession and IOAT in both eyes for infantile esotropia at 1 year of age. She was referred to our hospital for severe hypertropia of one eye. She showed 10 PD esotropia and 30 PD hypertropia of the right eye in the primary gaze. It worsened to 45 PD hypertropia of the right eye at the time of fixation with the left eye. On head tilt testing, 45 PD hypertropia of the right eye was shown with head tilt to the right side and 18 PD hypertropia of the right eye with head tilt to the left side.
IOOA 3+ in the right eye and -1.5 limitation of elevation in abduction and the primary gaze of the left eye were noted (Fig. 2-1). In FDT, slight upward resistance in abduction was detected. At the time of reoperation, we found mild adhesion between the IO and the surrounding tissues of the right eye. The IO was completely divided in two parts: the anterior half of the fiber was recessed 10 mm and the posterior half was preserved intact, revealing the original course with intact scleral insertion behind the LR. The status was incomplete IO recession of the right eye and IOAT of the left eye.
She was diagnosed with antielevation syndrome with limitation of elevation in the left eye due to IOAT and apparent IOOA of the right eye. The posterior half of the IO fiber was resected 10 mm to the point of the anterior half of the IO fiber in the right eye with 3 mm recession of the SR.
At 1 year postoperatively, IOOA of the right eye disappeared and esophoria of 10 PD was noted in the right eye (Fig. 2-2).
Discussion
In 1978, Scott9 first proposed the concept of IOAT by using a mathematical model. He described IOAT as the IO anteriorized to the level of scleral insertion of the IR, converting the function of the IO from elevation to depression and correcting hypertropia. Elliot and Nankin10 described IOAT in which the IO was adhered aside the insertion site of the IR. Since then, IOAT has been used for correction of IOOA and treatment of DVD or SOP.
Mims and Wood11 reported good effect of bilateral IOAT for the correction of DVD accompanied by marked IOOA. Elliot et al.10 specified that IOAT was a more effective IO weakening procedure than IO recession. The similar results were reported by Min and Park16,17 in the case of IOOA. Wright obtained good results from graded IO recession and IOAT.18,19 Since these reports, IOAT has been known to be the most effective when IOOA is associated with DVD.
IOOA and hypertropia can be treated with a single procedure, IOAT, in which the IO is attached anterior to the equator, changing the direction of the energy force of the IO from elevation to antielevation. However, a possible limitation of elevation in abduction and hypotropia in the primary position has been pointed out because the action of the IO after anteriorization is antielevation.
IOAT converted the function of the IO from elevation to depression, according to Scott.9 Stager20 speculated that the ligamentous structure of the neurofibrovascular bundle of the IO provided an ancillary origin for the posterior temporal fibers of the IO when its insertion was transposed anteriorly. Kushner12 suggested that limitation of elevation in the superotemporal gaze after IOAT was due to the effect of antielevation, not conversion of IO function from elevator to depressor.
Mims and Wood11 reported antielevation syndrome in 14 of 123 patients who underwent bilateral IOAT by them, and 2 of 77 patients by Kushner. Pseudo IOOA of the contralateral eye in antielevation syndrome following IOAT developed more after unilateral IOAT. Stein and Ellis14 said that the elevation of one eye, especially more in abduction, was limited by unilateral IOAT. Limitation of elevation induces more innervation to the SR in the same eye to elevate the eye. This stimulates yolk muscle in the contralateral eye according to Hering's law and so pseudo-IOOA occurs in the contralateral eye. This phenomenon is more remarkable the more anterior the IO is located to the equator. IOOA of the contralateral eye after surgery developed more prominently in the order of IOAT, 10 mm recession of the IO, and 14 mm recession of the IO.
Bremer et al.21 reported cases of hypotropia, limitation of elevation in abduction, and diplopia without findings of adherence syndrome after unilateral IOAT. Kim et al.22 reported two cases showing depression in abduction after IOAT, and Kim and Lee23 described a case of pseudo-IOOA of the opposite eye without any treatment. Mims and Wood11 and Ziffer et al.24 recommended performing IOAT bilaterally in cases of bilateral IOOA to prevent monocular limitation of elevation.
In this study, all of 7 patients underwent unilateral IOAT. In 4 patients, IOAT was performed in the contralateral eye resulting in symmetric IOAT in both eyes. Our successful result also shows that performing symmetric IOAT in both eyes is mandatory.
Case 2 (patient No. 5) underwent 10mm recession of the IO in the right eye and IOAT in the left eye. However, the anterior half of the IO of the right eye only was recessed and the posterior half was preserved intact in its original course, which produced the status of unilateral IOAT. The posterior fibers were resected 10 mm to fit to the anterior half fibers accompanied with 3 mm recession of the SR in the right eye.
In one patient (patient No. 6) with severe limitation of elevation in abduction and primary position, the previously anteriorized IO was extirpated without denervation. In another patient (patient No. 8) who did not show severe hyperdeviation of the apposite eye in primary gaze, the antielevating effect was reduced by 4 mm recession of the IO from the site of previous IOAT (Table 2).
Parks25 emphasized the possibility of adherence syndrome after IO weakening procedures, in which hypotropia, limitation of elevation in primary gaze, and positive FDT resulted in adhesion between surrounding tissue and the IO. Cho et al.26 reported 3 patients with adherence syndrome after IO weakening procedures. Hypotropia in primary gaze or severe adhesion around the IO is not found in antielevation syndrome, unlike adherence syndrome which arises from all kinds of IO surgeries.
In our patients, adherence syndrome could be ruled out because there was no hypotropia in primary gaze or resistance in FDT except the superotemporal direction. The resistance of the superotemporal direction was caused by a neurofibrovascular bundle, which was five times higher in tensile force than the SO tendon.27
The whole insertion of the IO to the sclera anterior or temporal to the IR insertion causes stretching of the neurovascular bundle located at the lateroposterior part of the IO, and excessive antielevation is frequently developed. To reduce antielevation, various methods for IOAT were designed. Kushner12 speculated that attaching the IO more than 2 mm anterior or more lateral to the IR insertion or the spread of IO insertion, might induce excessive limitation of elevation accompanied by severe excyclotorsion of the opposite eye. He recommended that the anterior fiber of the IO should be attached within 1 mm anterior to the IR insertion and the posterior fiber should be attached within 5 mm temporal from the lateral end of the IR. Others28,29 reported that a good corrective effect by modification of IOAT was obtained by locating the anterior fibers of the IO 2 mm anterior to IR insertion and the posterolateral fibers posterior to the lateral end of IR insertion or by performing J-deformity IOAT.
Cho15 describes a modified IOAT in which only the anterior 1/3 of the IO is attached to the lateral end of the scleral insertion of the IR, and the posterior 2/3 is naturally leaving without any attachment to the sclera. Excessive antielevation may be avoided by creating a small insertion of the IO and unstretching the posterior fiber. We used Cho's method15 in our patients and found that antielevation syndrome developed in 4 of 20 patients who had undergone unilateral IOAT (20%). This incidence is relatively low after unilateral IOAT.
Four referred cases underwent contralateral IO myectomy, IO extirpation without denervation, contralateral IOAT, and IO recession respectively. They obtained comitancy of binocular motility.
Unilateral IOAT performed for unilateral DVD and SOP may induce antielevation on abduction and the contralateral IOOA, and this may frequently cause incomitancy of version. Antielevation syndrome after unilateral IOAT can be managed by creating balanced antielevation in both eyes. Sometimes, this can be achieved by conversion of the IO to its position of recession or extirpation, to reduce the anti-elevating force. In bilateral IOAT, it is important to induce the balance of version by producing symmetric antielevation in both eyes.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






