


Fujii et al. [1] first introduced a 25-gauge transconjunctival sutureless pars plana vitrectomy system in 2002. Since then, microincision vitrectomy systems and instruments have evolved substantially. Microincision vitrectomy has also emerged as the mainstream approach for vitreoretinal surgery due to its advantages over conventional 20-gauge vitrectomy, including faster wound healing, faster visual recovery, fewer complications, and a decreased postoperative inflammatory response [2,3].
With the continued introduction of smaller gauge vitrectomy systems, vitrectomy probes have evolved to overcome the limitations of a decreased flow rate due to the narrower internal diameter. First, the port size of the vitrectomy probe was widened [4]. Development also focused on increasing the vacuum and maximum cutting rate [5]. Recently, vitrectomy probes with maximum cutting rates exceeding 7,500 cuts per minute (CPM) have become predominant. To adjust the duty cycle to increase the opening time of the port, the operating mechanism of the vitrectomy probe has evolved from a conventional spring system to a dual pneumatic system [6]. Dual cutting action vitrectomy probes with dual blades have also been introduced.
Until recently, various manufacturers have released various ultrahigh-speed vitrectomy probes with different performance and maximum cutting rates. Vitrectomy probes from the same manufacturer are compatible with the same vitrectomy system, which means there is a broader range of choices available for gauge selection and vitrectomy probe products that can be used for vitrectomy surgery. However, there has been a lack of research comparing the performance of various types of vitrectomy probes in practical vitrectomy settings. This study aimed to compare the efficiency and safety of various ultrahigh-speed dual pneumatic vitrectomy probes that are currently commercially available; specifically, those available in our institution.
Materials and Methods
Ethics statement
This study adhered to the principles of the Declaration of Helsinki and received approval from the Institutional Review Board of Soonchunhyang University (No. 2023-07-025). The requirement for informed consent was waived due to the retrospective nature of the study.
Patients
From the sample pool, all patients who underwent microincision three-port pars plana vitrectomy by a single operator (KSC) for idiopathic epiretinal membrane at Soonchunhyang University Seoul Hospital (Seoul, Korea) from March 2020 to February 2023 were included. Considering various factors such as the degree of vitreous liquefaction and posterior vitreous detachment (PVD), patients with an axial length of below 21.00 mm or above 26.50 mm, asteroid hyalosis, vitreous hemorrhage, diabetic retinopathy, retinal detachment, and those under 50 years old were excluded. For data collection, patient medical records and recorded intraoperative videos were retrospectively analyzed.
Data
The patients were divided into four groups based on four types of vitrectomy probes that are currently used in surgery: 23-7500 (UltraVit, Alcon Laboratories; 23-gauge 7,500 CPM), 23-7500 (UltraVit 25-gauge 7,500 CPM), 25-10K (Advanced UltraVit, Alcon Laboratories; 25-gauge 10,000 CPM), and 27-10K (Advanced UltraVit 27-gauge 10,000 CPM). For each group, data were collected and organized in terms of axial length measured using partial coherence interferometry (IOLMaster 700, Carl Zeiss Meditec), vitrectomy time, number of sutures performed, the occurrence of iatrogenic retinal breaks during surgery, postoperative hypotony (below 6 mmHg), retinal detachment, endophthalmitis, and other complications. The vitrectomy time was defined as the time taken to remove the vitreous within the maximum visible range using a noncontact wide angle viewing system (Resight, Carl Zeiss Meditec) without indentation. The time taken to change instruments and the time spent on other procedures during surgery, such as PVD induction and removing membranes, were excluded from the vitrectomy time.
Surgical procedures
A three-port pars plana vitrectomy was performed using the vitrectomy system (Constellation, Alcon Laboratories). All patients who had not previously undergone cataract surgery underwent combined cataract surgery.
In all surgeries, the vitreous was removed using a noncontact wide angle viewing system with a 128 diopters (D) lens, followed by membranectomy using a 60 D lens. When using the 23-7500 and 25-7500 probes, core vitrectomy was performed using a dual dynamic drive (three dimensional, 3D) mode at a moderate cutting rate, followed by peripheral vitrectomy at a high cutting rate (23-7500: 3,500-7,500 CPM, 250-450 mmHg; 25-7500: 3,500-7,500 CPM, 350-650 mmHg). When using the 25-10K and 27-10K probes, core and peripheral vitrectomy were performed using the proportional vacuum mode at high speed and a fixed cutting rate (0-650 mmHg). If the PVD was not present, the vitreous was visualized using triamcinolone acetonide (MaQaid, Wakamoto Pharmaceutical), and after PVD induction, vitrectomy was completed in all patients. Triamcinolone acetonide and indocyanine green were then used to visualize the epiretinal membrane and inner limiting membrane, respectively, for membranectomy and inner limiting membrane peeling.
After completing the manipulation of the posterior pole, the area around the vitreous base was examined with indentation to confirm the presence of retinal breaks or degenerations. If any were present, endolaser photocoagulation was performed. Finally, the cannulas were removed, and each sclerotomy site was checked for spontaneous closure. If any leakage was observed, single stitch with 8-0 polyglactin (Vicryl, Ethicon Inc) was used for each sclerotomy site to end the surgery.
Statistical analysis
All statistical analyses were performed using IBM SPSS ver. 23.0 (IBM Corp). The demographics and data for each group were analyzed using one-way analysis of variance and the Kruskal-Wallis method to determine significant differences among group data values. The occurrences of complications during surgery and after surgery were presented as percentages. Simple correlation analysis was applied to assess the correlation between axial length and vitrectomy time.
Results
This study included a total of 82 eyes from 82 patients, with 16, 11, 26, 29 eyes in the 23-7500, 25-7500, 25-10K, and 27-10K groups, respectively. There were no significant differences in the patients’ preoperative characteristics among the groups (Table 1).
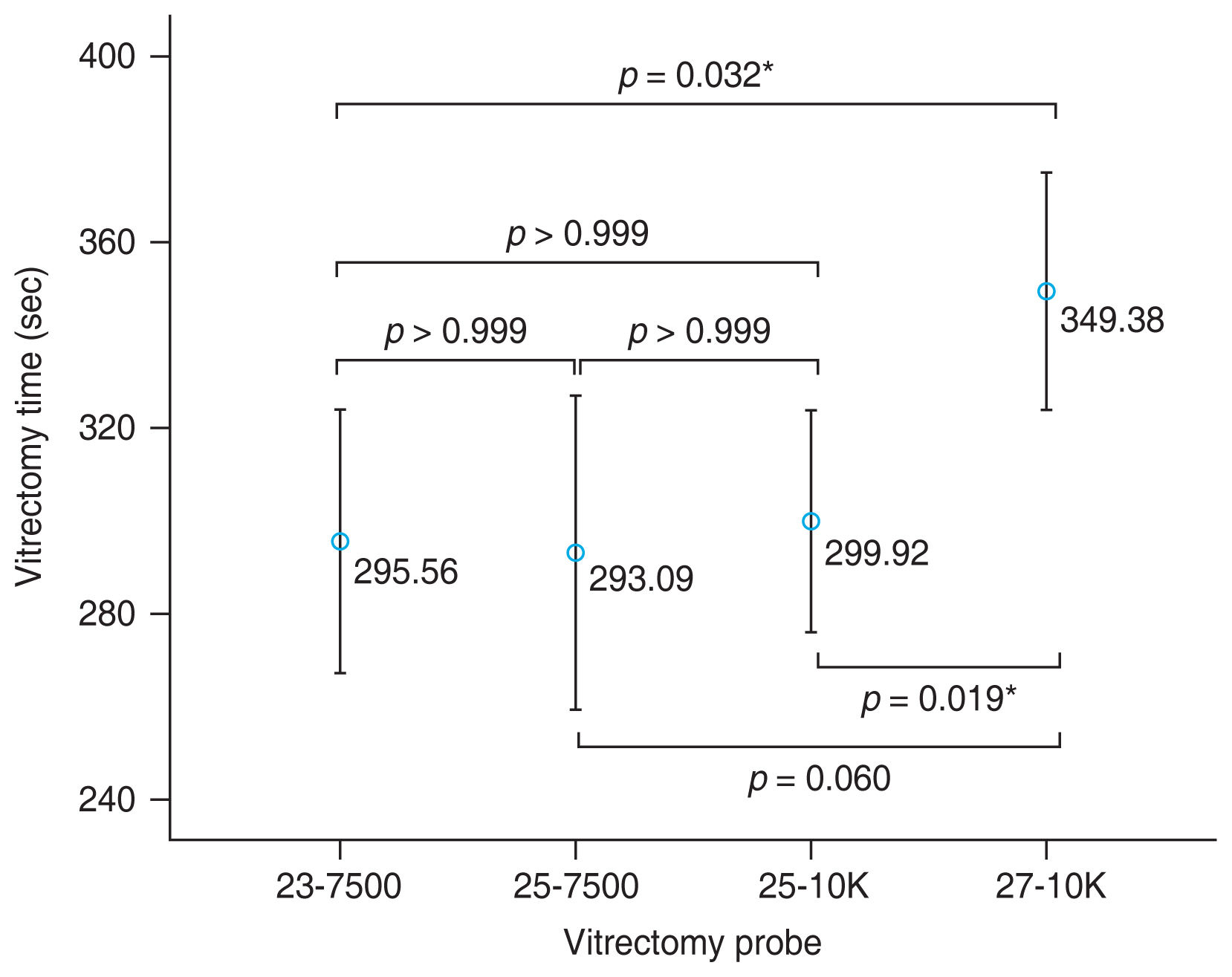
The vitrectomy time results for the 23-7500, 25-7500, 25-10K, and 27-10K groups were 295.56 ± 53.55, 293.09 ± 50.28, 299.92 ± 59.42, and 349.38 ± 67.23 seconds, respectively (Table 2). There was no significant difference among the 23-7500, 25-7500, and 25-10K groups in vitrectomy time. However, the vitrectomy time of the 27-10K group was longer than that of the other groups. But when compared to the vitrectomy time of the 25-7500 group, it did not show statistical significance (Fig. 1). There was no significant correlation between axial length and vitrectomy time in any of the four groups (23-7500 group, p = 0.174; 25-7500 group, p = 0.552; 25-10K group, p = 0.077; 27-10K group p = 0.220).
The mean numbers of sutures required to close the sclerotomy sites were 3 for the 23-7500 and 25-7500 groups, 2.96 for the 25-10K group, and 0.83 for the 27-10K group. Iatrogenic retinal breaks occurred during surgery in one eye in the 23-7500 group, and postoperative hypotony occurred in one eye in the 27-10K group. No cases of retinal detachment or endophthalmitis occurred after surgery in any group (Table 3).
Discussion
In recent years, microincision vitrectomy has evolved with the introduction of 23-, 25-, 27-gauge systems. Even when using the same gauge, vitrectomy probes have also improved in terms of efficiency and safety. One measure of vitrectomy efficiency is the time taken for vitreous removal, which is affected by factors such as vitreous viscosity, the size of fragmented vitreous, cutting rate, duty cycle, inner diameter, and port size of the vitrectomy probe [4,7,8]. The flow rate can also serve as a measure of vitrectomy efficiency with a higher average flow rate of vitreous during vitrectomy resulting in shorter vitrectomy time.
The probes used in this study were UltraVit and Advanced UltraVit, both of which are single-blade probes that are operated using a dual pneumatic system. However, the Advanced UltraVit probe offers an enhanced maximum cutting rate, increasing from 7,500 to 10,000 CPM compared to the UltraVit probe. For the 25-gauge probe, the port size increased from 0.015 to 0.016 inches. Further, the tip of the probe is beveled, which allows the probe to approach closer to the retina [9]. When aspirating vitreous, the port of the vitrectomy probe can be obstructed due to the viscosity of the vitreous, thus increasing the internal resistance within the probe. As the cutting rate increases, the vitreous is cut into finer fragments, which reduces internal resistance within the probe and turbulence around the tip. Consequently, a higher cutting rate can lead to an increase in vitreous flow rate [10,11]. Therefore, vitrectomy probes are now being developed with maximum cutting rates up to 20,000 CPM.
As the gauge increases to 27-gauge, the safety of fluid dynamics improves and the traction exerted on the retina decreases, ultimately enabling safer surgery. Furthermore, the smaller diameter of the sclerotomy site associated with higher gauges is expected to seal better and reduce the risk of postoperative hypotony. Saleh et al. [12] demonstrated that the occurrence of postoperative hypotony was lower in the eyes using the 27-gauge system compared to those using the 23-gauge system. However, there is a limitation in terms of the benefits associated with increasing the gauge, in that the resistance of fluid flow through the narrowed lumen increases, thus resulting in lower flow rate [13]. This is in accordance with the Poiseuille law, where the velocity of a Newtonian fluid is inversely proportional to the resistance within the conduit and resistance is inversely proportional to the fourth power of the conduit radius. Although vitreous is a non-Newtonian fluid containing collagen fibers and hyaluronic acid and therefore does not fully obey Poiseuille law, reducing resistance within the vitrectomy probe is more crucial when aspirating vitreous with smaller gauge instruments [14].
Recently, several studies have compared fluid flow rates when aspirating balanced salt solution (BSS) using various vitrectomy probes, but it is important to note that the vitreous and BSS have distinct compositions. The complex nature of vitreous is unpredictable during vitrectomy, which can occasionally result in variations in the vitrectomy time generating a high standard deviation due to vitreous flow obstruction [15]. In this study, the 27-10K probe showed inferior vitrectomy times compared to groups using other probes. This might be attributable to the fact that, despite advancements in vitrectomy probe technology, the inner diameter of the 27-gauge probe (0.0096 inches) did not surpass the dimensions of the 23-gauge probe (0.0141 inches) or the 25-gauge probe (0.0116 inches). The absence of a significant difference in vitrectomy time between the 23- and 25-gauge groups, despite differences in inner diameter, could be due to the surgeon being cautious while using the 23-gauge probe, considering the force exerted on the vitreous fibers and retinal tissue. In fact, experimental studies using cantilever apparatus with latex membranes have shown differences in area of influence during tissue attraction between 23- and 25-gauge probes [16,17]. The surgeon also experienced more vitreous fluctuations on the vitreoretinal surface when using 23-gauge probes compared to 25-gauge probes, and this study recorded an instance of an iatrogenic retinal break during peripheral vitrectomy using the 23-gauge probe. It is also believed that the enlarged port of the 25-gauge vitrectomy probes could have an effect.
Experimentally, the 25-10K probe exhibited a higher flow rate than the 25-7500 probe [9]. However, as documented in the study of Patel et al. [18], this study also did not find a significant difference in vitrectomy time between these two groups in the clinical setting. This could largely be attributable to the same inner diameter size, and the 7,500 CPM probe already achieved a much shorter vitrectomy time (higher flow rate) compared to the previously released 5,000 CPM probe [19]. The difference between 3D mode and proportional vacuum mode therefore likely had an impact. The 3D mode adjusts cutting rate and vacuum in a linear manner, thus creating a vitreous flow to enhance efficiency. When surgeons press the foot pedal, the cutting rate gradually changes to a preset starting point, and the vacuum increases to its maximum point. By contrast, proportional vacuum mode linearly adjusts vacuum at a fixed high cutting rate. This can reduce pulsatile traction and enhance safety. Using 3D mode, core vitrectomy can be performed quickly with a low cutting rate and high vacuum. When using proportional vacuum mode, the authors suggest that maintaining 10,000 CPM for vitreous removal may require a bit more time, because, with the reduced pulsatile traction and the enhanced safety, surgeons need to approach remaining vitreous more closely to remove it [6].
In experimental studies, the performance of probes is typically compared by removing a certain amount of BSS. However, in practice, the volume of vitreous can vary between individuals, which is believed to affect vitrectomy time. Some studies, using methods such as computed tomography or measuring the volume of the fluid filling the vitreous cavity after vitrectomy, have reported a significant correlation between axial length and vitreous volume [20-22]. Therefore, in this study, cases with excessively short or long axial length were excluded, and no significant correlation was found between axial length and vitrectomy time in any of the four groups.
In all small gauge systems, cases of hypotony due to unsutured wound leakage after surgery are rare, and even if it does occur, it often recovers within a week, without severe complication like choroidal detachment or hypotony maculopathy; therefore, the sclerotomy sites are often not sutured [23,24]. However, even though the reported occurrence rates of postoperative hypotony were low, the incidence has varied across studies, so the author preferred to suture sclerotomy sites. For 23-gauge, all 0.64 mm diameter sclerotomy sites were sutured, while for 25-gauge, the 0.51 mm sclerotomy sites were sutured if there was even a slight leakage. Given the notably smaller 0.40 mm diameter of the 27-gauge sclerotomy site, the need for suturing was minimal. Consequently, no cases of hypotony were observed in the 23-7500, 25-7500, and 25-10K groups, and in the 27-10K group, there was one instance of intraocular pressure that decreased to 6 mmHg on the first day after surgery. However, this case did not involve severe complications such as choroidal detachment or hypotony maculopathy, and the intraocular pressure subsequently normalized without any special treatment. Aside from this case, there were no other postoperative complications such as retinal detachment or endophthalmitis in any of the groups.
This study has several limitations. First, due to its retrospective nature, there was an uneven distribution of each probe, and the relatively small sample size could also represent a limitation. Further, although the liquefaction degree of the vitreous or the extent of PVD could influence the vitrectomy time, these factors were not fully considered, because it is difficult to quantify the degree of the vitreous liquefaction and the extent of PVD, even when using B-scan ultrasonography. Further, in calculating vitrectomy time, we reviewed the recorded video and analyzed it in second level counts whenever there was a change in instrument or procedure, thus resulting in imprecise aggregation of some fractions of seconds. Although the effect that the difference in the vitrectomy mode (3D and proportional vacuum) can have on the vitrectomy time result was mentioned above, not controlling the variable of vitrectomy mode is another limitation of this study.
In conclusion, three types of probes, 23-7500, 25-7500, and 25-10K, showed no significant differences in vitrectomy time or intraoperative or postoperative complications. While showing improved performance, the 27-10K probe still exhibited the physical limitation of a narrow 27-gauge compared to the other three types of probes. However, although the perceived vitrectomy time with the ultrahigh-speed 27-gauge small diameter probe may seem much longer than with the larger diameter probes, the actual difference was less than a minute on average, and it has the advantage of reduced traction on the retina resulting in fewer iatrogenic breaks. Further, the patient’s discomfort after surgery might be minimized due to the reduced need for suturing in many cases, even when considering strict criteria. Therefore, it is reasonable to choose smaller gauge probes with increased cutting rates based on the surgeon’s preference. However, this study primarily focused on vitrectomy time. Other factors including noise, vibration fatigue in the hands due to the higher cutting rate, and the low rigidity of surgical instruments such as intraocular forceps and endolaser probes are likely to serve as more significant obstacles than vitrectomy time in the selection of 10,000 CPM 27-gauge vitrectomy probes.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Download Citation
Download Citation Print
Print






