Postoperative Refractive Outcomes of Biometric Formulas in Phacovitrectomy with Gas Tamponade
Article information
Abstract
Purpose
To investigate the refractive accuracy of intraocular lens (IOL) power calculation for biometric formulas in phacovitrectomy.
Methods
This retrospective study included 357 eyes of 357 patients who underwent phacovitrectomy using four commonly available IOL power formulas: Hoffer Q (87 eyes), Holladay 1 (78 eyes), Holladay 2 (91 eyes), and SRK/T (101 eyes). The mean refractive error (ME) and the mean absolute refractive error (MAE) were calculated based on the predicted postoperative refraction error, and they were compared using analysis of variance test. Subjects were divided into high myopic eyes (axial length, ≥26 mm) and nonhigh myopic eyes (axial length, <26 mm).
Results
The ME and the MAE after phacovitrectomy did not show a significant difference among the four IOL power formulas (p = 0.546 and p = 0.495, respectively). There was no significant statistical difference in formulas when the eyes were grouped into high myopia and nonhigh myopia (ME: p = 0.526 and p = 0.482, respectively; MAE: p = 0.715 and p = 0.627, respectively). The ME showed myopic shift in all formulas regardless of IOL formula used. The ME showed greater myopic shift in high myopia group than nonhigh myopia group in all formulas.
Conclusions
Our study did not find evidence for superiority of any formula in phacovitrectomy. However, in phacovitrectomy, possible myopic shift should be considered for IOL power calculation. Especially, in phacovitrecotmy in patients with high myopia, more myopic shift should be considered when selecting IOL.
Phacovitrectomy, a combined surgery of phacoemulsification and intraocular lens (IOL) placement with pars plana vitrectomy (PPV), has become a common useful procedure for patients with vitreoretinal disorder and a coexisting cataract [1–4]. With the anatomical success of phacovitrectomy, greater attention has been given to enhancing postoperative refraction [5–8]. To obtain ideal outcomes, accurate IOL power calculation formulas and precise biometric measurements need to be performed in advance; however, IOL power calculation and axial length (AL) determination with ultrasound biometry are possible sources of miscalculation [6].
Several IOL power calculation formulas are generally available. The representative formulas are SRK/T, Holladay 1, Holladay 2, and Hoffer Q [9,10]. These formulas are third-generation formulas that merge theoretical eye models with linear regression methods. These formulas predict the effective lens position by performing calculations based on AL and keratometry data variables. Each formula employs different expressions for accurate calculation of the effective lens position. The SRK/T formula uses “A constant,” which is based on multiple variables. Holladay 1 uses a personalized surgeon factor called S factor, and Hoffer Q uses a personalized anterior chamber depth value. These IOL formulas were created using algorithms derived from large sets of clinical data from cataract operation, and thus, their accuracy may be different when used for IOL power calculations after phacovitrectomy. In addition, all these four formulas use AL, keratometry, and anterior chamber depth as common parameters, all of which are possibly influenced by the phacovitrectomy procedure [11,12].
Accurate IOL measurement can provide a better vision for patients, so people have been doing a lot of research to predict the correct IOL calculation. There are studies that evaluated the accuracy of the IOL in the nonvitrectomized eyes that performed cataract surgery alone and the vitrectomized eyes [13–16]. there are studies showing that myopic shift appeared in the eyes after phacovitrectomy, and studies showing that there was no myopic shift after phacovitrectomy [17–19]. However, the research is almost rare for examining the comparative accuracy of IOL power calculation formulas in phacovitrectomy, although there have been reports of refractive outcomes in phacovitrectomy. Therefore, we investigated the accuracy of the commonly available IOL calculation formulas, including Hoffer Q, Holladay 1, Holladay 2, and SRK/T, after phacovitrectomy.
Materials and Methods
Ethics statements
This study was approved by the Institutional Review Board of St. Vincent’s Hospital, The Catholic University of Korea (No. VC10RISI0135). This study was conducted in accordance with the principles of the Declaration of Helsinki. The requirement for informed consent was waived due to the retrospective nature of the study.
Study subjects
The retrospective study was performed using patients who had combined surgery of phacoemulsification and foldable IOL placement with PPV for stage 3 or 4 macular hole between 2007 and 2013 at the Catholic Medical Center, The Catholic University of Korea (Seoul, Korea). The exclusion criteria were as follows: eyes with corneal disease such as keratoconus, corneal dystrophy, IOL insertion into the sulcus, scleral IOL fixation, retinal detachment, silicone oil injection, previous intraocular surgery, history of acute angle closure glaucoma, uveitis, pseudoexfoliation syndrome, posterior iris synechia, and previous trauma.
Clinical examinations and outcome measures
The experienced optometrists performed the preoperative biometry and measured the postoperative refractive errors. All of the enrolled patients underwent objective refraction assessments using an autorefractor (RK-5 Auto-Ref-Keratometer, Canon), intraocular pressure mensuration, slit-lamp examination, fundus photography, and ultrasonographic B scan prior to the procedure. The AL was computed by ultrasonographic A scan (Echograph model axis II, Quantel Medical). Keratometry (Topcon DM-4, Topcon) and autorefraction were measured both preoperatively and 4 months postoperatively. Refractive error was measured three times and the average value was used. The subjects were classified into two groups depending on the AL: nonhigh myopic eyes (AL, <26 mm) and high myopic eyes (AL, ≥26 mm). The patients were classified into four groups according to the four commonly available IOL power formulas used in phacovitrectomy (SRK/T, Holladay 1, Holladay 2, and Hoffer Q). The IOL power formula used in phacovitrectomy was randomly chosen by the surgeon’s preference. The mean refractive error (ME) was calculated as the difference between expected spherical refraction and actual spherical equivalent of postoperative refraction. The mean absolute refractive error (MAE), which is the absolute value of the ME, was also estimated. The cutoff of myopic shift was defined as −0.5 and −1.0 diopters, respectively. To verify a significance of the ME and MAE between four formulas, one-way analysis of variance testing was executed by SPSS ver. 17.0 (SPSS Inc). A value of p < 0.05 was considered statically significant.
Surgical technique
Surgical procedure was performed by single experienced expert retinal surgeon (DJ). The patients were prepared for general or retrobulbar anesthesia (lidocaine and bupivacaine, 6:4 mixed solution). After creating three sclerotomies by a 23-gauge trocar, a 3-mm temporal clear corneal incision was made with insertion of viscoelastic material. A 5.0- to 5.5-mm continuous curvilinear capsulorhexis was created by using forceps. Phacoemulsification was done using stop-and-chop technique, and irrigation and aspiration were executed to extract the residual cortex. A foldable IOL (AcrySof IQ SN60WF, Alcon Inc) was placed into capsular bag using cartilage introduction method, without expansion of the corneal wound. The viscoelastic liquid substance was taken out afterwards. A standard three-port PPV was conducted by an Accurus 23-gauge system (Alcon Inc), and internal limiting membrane (ILM) was removed using indocyanine green dye by ILM forceps. A 14% perfluoropropane gas tamponade used to refill the vitreous cavity. After trocars were removed, no suture was required for sclerotomy site reapproximation.
Results
The records of 385 patients (385 eyes) who underwent phacovitrectomy for macular hole were reviewed. After excluding nine patients with IOL sulcus insertion, eight patients with incomplete closure of macular hole, five patients with posterior iris synechia, and six patients who were unable to follow-up, we enrolled 49 high myopic patients and 308 nonhigh myopic patients in this study. Demographic characteristics are shown in Table 1.

Clinical characteristics of subjects according to the intraocular lens calculation formula types in the study
Table 2 shows that there were no significant differences in the ME calculated by all four formulas (p = 0.546), and no difference when eyes were stratified as nonhigh myopic eyes and high myopic eyes (p = 0.482 and p = 0.526, respectively). The ME showed myopic shift in all formulas.
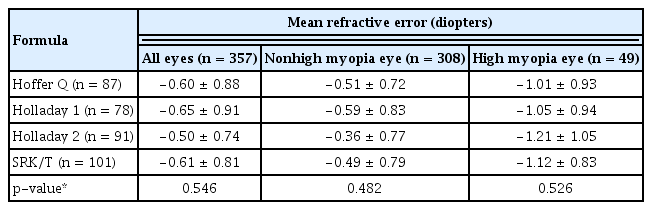
Comparison of mean refractive error calculated by the four intraocular lens formulas
The ME showed greater myopic shift in high myopic eye group than nonhigh myopic eye group, in all formulas. Table 3 shows that there were no significant differences in the accuracy of the four formulas in the prediction error measured by the MAE (p = 0.495). Further, no difference was illustrated in either the high myopic eye group or the nonhigh myopic eye group (p = 0.627 and p = 0.715, respectively).

Comparison of mean absolute refractive error calculated by four intraocular lens formulas
As shown in the Table 4, the percentage of the refractive error within ±0.50 diopters of the planned refraction were highest in the Holladay 2 (39.6%), and lowest in the Holladay 1 (23.1%) formulas. Specifically, the percentage of the refractive error within ±0.50 diopters of the planned refraction was highest in the Holladay 2 formula (42.0%) in nonhigh myopic eyes.

Percentage of eyes achieving the planned refraction
Discussion
Our study did not find evidence for superiority of any formula in phacovitrectomy. The Hoffer Q, Holladay 1, Holladay 2, and SRK/T formulas did not show a significant statistical difference of refractive error after phacovitrectomy. However, the ME showed myopic shift in all four formulas, regardless of IOL formula used. Additionally, we found that the ME showed greater myopic shift in high myopia than nonhigh myopia.
The reasons for these results in our study can be explained by several possibilities. several confounding factors of phacovitrectomy, in contrast to simple cataract surgery, may have affected the accuracy of the IOL calculation formulas. First, there is a possibility that the IOL may move forward due to the influence of gas, intraocular filling material, after phacovitrecotmy. Second, the interaction between the lens and vitreous disappears after phacovitrectomy, which may cause a change in the anterior chamber depth, resulting in refractive errors. Third, in phacovitrectomy, since the trocars are inserted into pars plana in front of equator, the incisional sites of the sclera may be vulnerable to pressure changes, which can increase the AL of eyeball in the process of healing the wound. Fourth, it is possible that the preoperative AL of the eye-ball was underestimated. Our study was conducted in patients with macular hole. Macular hole is caused by vertical vitreoretinal traction and tangential traction. Vertical vitreoretinal traction can lead to underestimation of AL.
Our study found that in all formulas, high myopic eyes exhibit greater myopic shift than nonhigh myopic eyes for refractive error after phacovitrectomy. It is thought to be a meaningful finding that all formulas showed same trend in high myopic group. one possible explanation is hypothesis that high myopic eyes can be more susceptible to pressure forces due to thinner sclera. These forces may lead to a true more increase of AL. Sclera contains mainly collagen and some crucial elastic fiber. Thinning of sclera in highly myopia is associated with dissociation of collagen fiber bundles and reduction of collagen fiber diameter. There are also differences in the biochemical composition of sclera, such as changes in content of glycosaminoglycan and collagen [20,21]. These facts can reduce stiffness of sclera and decrease stability in highly myopic eyes, for intraoperative and postoperative pressure and stress. Consequently, it may cause more increase in AL and eventually cause more myopia shift in the high myopic eyes compared to the nonhigh myopic eyes. We did not find statistical difference in refractive error among the four formulas. However, postoperative ocular AL could not be measured in our study. So, it is just a hypothesis. Further future studies using postoperative ocular length are needed.
Several studies have been conducted on refractive prediction error after phacovitrectomy. It has been reported that the IOL power calculation formulas after phacovitrectomy are less accurate than those used after simple cataract surgery [9,10,22]. Shiraki et al. [23] compared the group that underwent cataract surgery alone with the group that did not inject gas after phagovitrectomy, and the group that injected gas after phacovitrectomy. They showed that greater myopia shift in gas injection group, due to the change of the forward movement in IOL position. These results support our results. However, in the study by Katz et al. [24], there was no difference in refractive error between intraocular fillings (gas, air, and balanced salt solution). Hotte al. [25] reported that preoperative AL is an independent predictor of postoperative myopic refraction error in multivariate analysis, and conversely, other studies [24,26] described that there was no change in AL after phacovitrectomy. It is difficult to predict the pattern of change of these parameters and this may reduce the accuracy of refractive outcomes among the formulas. Further studies are needed to verify these hypotheses.
The major strength of the present study is that four different formulas were analyzed, unlike previous studies that used only one formula [18,19,24,26]. Another strength is that one expert operator performed all the surgeries and implant the same kind of IOL. Moreover, we analyzed data by dividing it according to the AL of the eyeball.
This study has some limitations, including retrospective research. We have not investigated the visualization of dynamics such as tilting and decentration that the position of IOL may be unstable due to lack of vitreous support. We could not quantify for the hypotheses of postoperative anterior shift of the IOL plane, postoperative AL elongation due to lack of postoperative examination. And we used ultrasonographic A scan, which is less accurate than optical biometrics. Currently, optical biometry such as IOL master are usually being used. Further future research is needed using optical biometry. Also, there is a limitation that we chose the IOL formula according to the operator’s preference. In clinical practice, the IOL formula is chosen differently depending on AL. However, there are various differences in the accuracy of the IOL formula according to AL in each study. In this study, IOL formula according to AL was not selected, and it is thought that further research is needed. Nevertheless, it is thought to be significant that our findings showed the same tendency of greater myopic shift in high myopia in all four formulas, after phacovitrectomy.
In conclusion, our study did not find evidence for superiority of any formula in phacovitrectomy. However, in phacovitrectomy, possible myopic shift should be considered for IOL power calculation. Especially, in phacovitrecotmy in patients with high myopia, more myopic shift should be considered when selecting IOL. Given that no formulas have been developed specifically for phacovitrectomy, further studies are needed in order to develop accurate IOL power calculations after phacovitrectomy.
Acknowledgements
None.
Notes
Conflicts of Interest: None.
Funding: None.