Experimental Assessment of the Performance of Dual Pneumatic Vitreous Cutters According to Gauge and Cut Rate
Article information
Abstract
Purpose
To compare and analyze the performance of dual pneumatic ultra-high-speed vitreous cutters based on their cut rates, vacuum levels, and diameters in terms of flow rate and cutting time.
Methods
The Constellation Vision System was used to remove egg white for 30 seconds, after which we calculated the flow rate by measuring the change in weight. We then measured the time required to remove 4 mL of egg white. We tested the UltraVit (UV) 7,500 cuts per minute (cpm) probe and the Advanced UltraVit (AUV) 10,000 cpm probe in biased open duty cycle mode, using 23-, 25-, and 27-gauge probes, respectively.
Results
In biased open duty cycle, the flow rate tended to decrease as the cut rates increased for all three gauges. At the same cut rates, the flow rate increased as the vacuum level increased (p < 0.05), and as the diameter increased (p < 0.05). Among cutters with the same diameter, the AUV cutter showed higher flow rates than the UV cutter, with increases of 0.267 mL/ min (18.5%) at 27 gauge, 0.627 mL/min (20.8%) at 25 gauge, and 1.000 mL/min (20.7%) at 23 gauge (all p < 0.05). The times required to remove 4 mL of egg white took longer with the UV cutter than the AUV cutter for all three gauges (all p < 0.05).
Conclusions
The use of a smaller gauge vitreous cutter may reduce the flow rate and increase the time required for vitrectomy, but this can be partially compensated for by increasing the vacuum level as well as using a vitreous cutter with a higher maximum cut rate, improved port size, and improved duty cycle.
In 1971, Machemer et al. [1] introduced the vitreous infusion suction cutter and devised pars plana vitrectomy for vitreous removal, which has since come to be the most commonly used surgical procedure for vitreoretinal diseases. The evolution of vitrectomy has progressed with two main goals: miniaturizing the port and increasing the cut rates. Port miniaturization has allowed for less invasive surgery, thus reducing patient discomfort after surgery. Increasing the cut rates has allowed for more efficient vitreous removal with less traction and greater fluid stability [2–5].
During vitrectomy, the flow rate is affected by various factors, such as the viscosity of the vitreous, the cut rate, the duty cycle (the percentage of time the port of the vitreous cutter is open during one cutting cycle), and the shape of the vitreous cutter [6]. Therefore, better control of these factors leads to safer and more efficient surgery. Conventional spring-return pneumatic vitreous cutters use air to close the port and spring force to reopen it, which limits the control of the duty cycle [5]. This causes as the cut rate increase, the duty cycle to decrease, and the flow rate to ultimately decrease as well. By contrast, dual pneumatic vitreous cutters use two separate tubes to open and close the port, thus allowing the port to be opened and closed by the force of air in different tubes, which makes it relatively easy to control the duty cycle. The duty cycle can be selected from the following options: biased open (maximum port opening), 50/50 (port opens only 50% of the cutting cycle), or biased closed (minimum port opening) [7].
Increasing the cut rates of the vitreous cutter may result in finer vitreous fragments, therefore making vitreous aspiration easier and reducing the surge effect, but it can also affect the duty cycle. Decreasing the vacuum level weakens the force attracting the vitreous, which results in decreased acceleration of the fragmented vitreous entering the port of the vitreous cutter [6,8]. Therefore, the cut rates, duty cycle, vacuum level, and flow rate are all closely linked with each other [7].
This study aims to improve our understanding of commercially available vitreous cutters and provide information to aid in instrument selection for vitrectomy surgery.
Materials and Methods
The Constellation Vision System (Alcon Laboratories Inc) was used, and the UltraVit (UV; Alcon Laboratories Inc) 7,500 cuts per minute (cpm) vitreous cutter and the Advanced UltraVit (AUV; Alcon Laboratories Inc) 10,000 cpm vitreous cutter were tested while using 23, 25, and 27 gauges. The Constellation Vision System was set to the biased open duty cycle, which is the preferred duty cycle for core vitrectomy among the three selectable duty cycles (biased open, 50/50, and biased closed). For each vitreous cutter, combinations of cut rates of 500, 2,500, 5,000, 7,500 cpm, and up to 10,000 cpm for the AUV cutter were tested, along with vacuum levels of 250, 450, and 650 mmHg, and each setting was tested three times.
Egg white was placed in a vial and weighed on a precision (0.01g) balance. The weight loss was calculated for 30 seconds from the point at which the vitrectomy probe was completely immersed in the egg white and the preset cut rates and vacuum level were reached. The flow rate was calculated by dividing the weight loss (grams) by the product of the density of the egg white (assumed to be 1 g/mL) and the time (seconds) taken to achieve weight loss. This calculation was repeated three times for each setting, and the average value of these three calculations was used.
Moreover, the time required to remove 4 mL of egg white—which is similar to the actual vitreous humor volume—was measured using each vitreous cutter under the setting of the maximum cut rates and the maximum vacuum level in the biased open duty cycle. The average values for each cutter were calculated after repeating the experiment three times and then compared.
Statistical analysis was performed using IBM SPSS ver. 21.0 (IBM Corp), and p-values less than 0.05 were considered statistically significant. The Shapiro-Wilk test was used to check normality. Independent t-test and one way analysis of variance (ANOVA) with Tukey post hoc test was used to compare the groups as the data conformed to the normal distribution. Linear trend lines in Microsoft Excel (Microsoft Corp) were used to identify trends.
Results
The flow rates for each of the gauge cutters obtained under different cut rates and vacuum levels are depicted in Fig. 1A, 1B, 2A, 2B, 3A, and 3B. The values measured under each parameter are provided in Table 1. With both the AUV cutter and the UV cutter, the flow rate tended to decrease as the cut rates increased for all three gauges. At the same cutting rate, the flow rate increased as the vacuum level increased (one way ANOVA with Tukey post hoc test, all p < 0.05). The flow rates using the AUV cutters under the maximum cut rates and 650 mmHg vacuum were 1.707 ± 0.052 mL/min for 27 gauge, 3.640 ± 0.354 mL/min for 25 gauge, and 5.820 ± 0.317 for 23 gauge. Under the same cut rates and vacuum setting, the flow rates obtained using the UV cutters were 1.440 ± 0.090 mL/min for 27 gauge, 3.013 ± 0.230 mL/min for 25 gauge, and 4.820 ± 0.104 mL/min for 23 gauge. The flow rate decreased as the diameter decreased (one way ANOVA with Tukey post hoc test, all p < 0.05) (Fig. 4). Among cutters with the same diameter, the AUV cutter showed higher flow rates than the UV cutter, with increases of 0.267 mL/min (18.5%) at 27 gauge, 0.627 mL/min (20.8%) at 25 gauge, and 1.000 mL/min (20.7%) at 23 gauge (independent t-test, all p < 0.05).
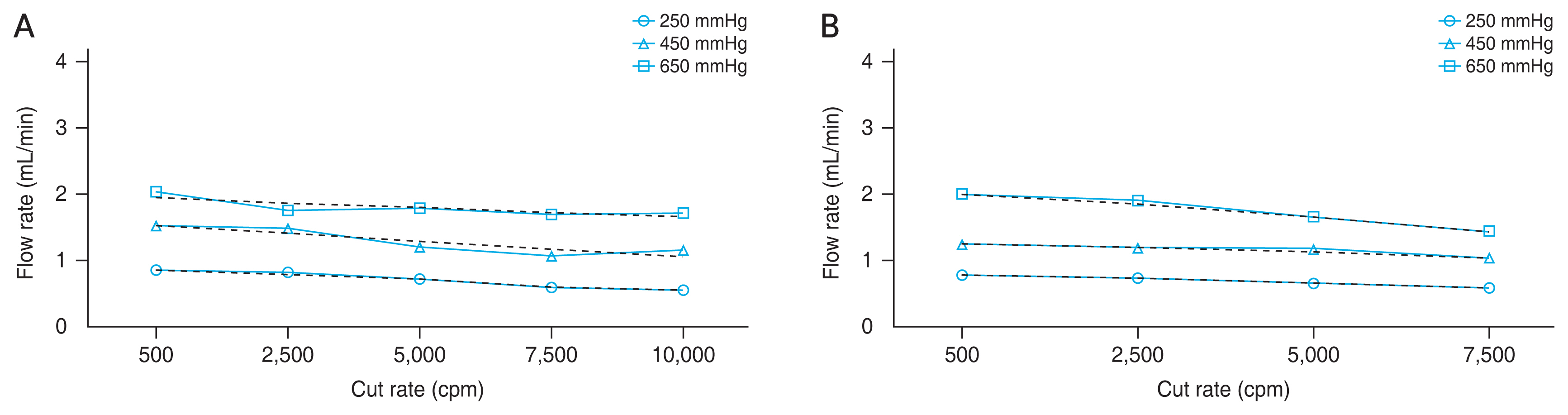
Egg white flow rates of 27-gauge vitreous cutters in biased open duty cycle. (A) Advanced UltraVit 10,000 cuts per minute (cpm) cutter. (B) UltraVit 7,500 cpm cutter. Each data point represents the average flow rate, and dashed lines indicate linear regression trends.
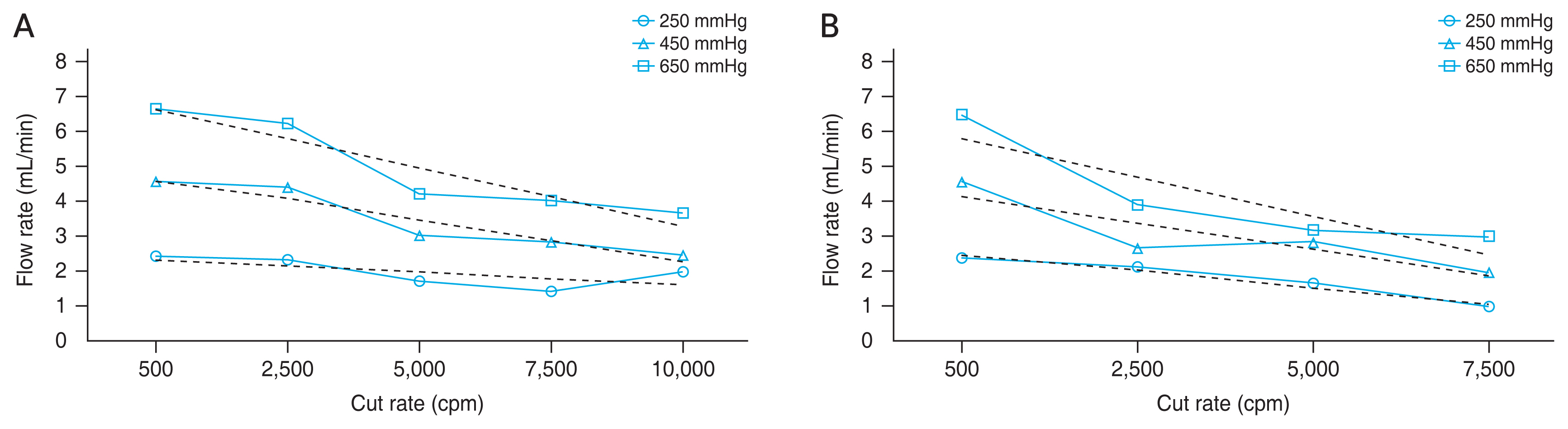
Egg white flow rates of 25-gauge vitreous cutters in biased open duty cycle. (A) Advanced UltraVit 10,000 cuts per minute (cpm) cutter. (B) UltraVit 7,500 cpm cutter. Each data point represents the average flow rate, and dashed lines indicate linear regression trends.
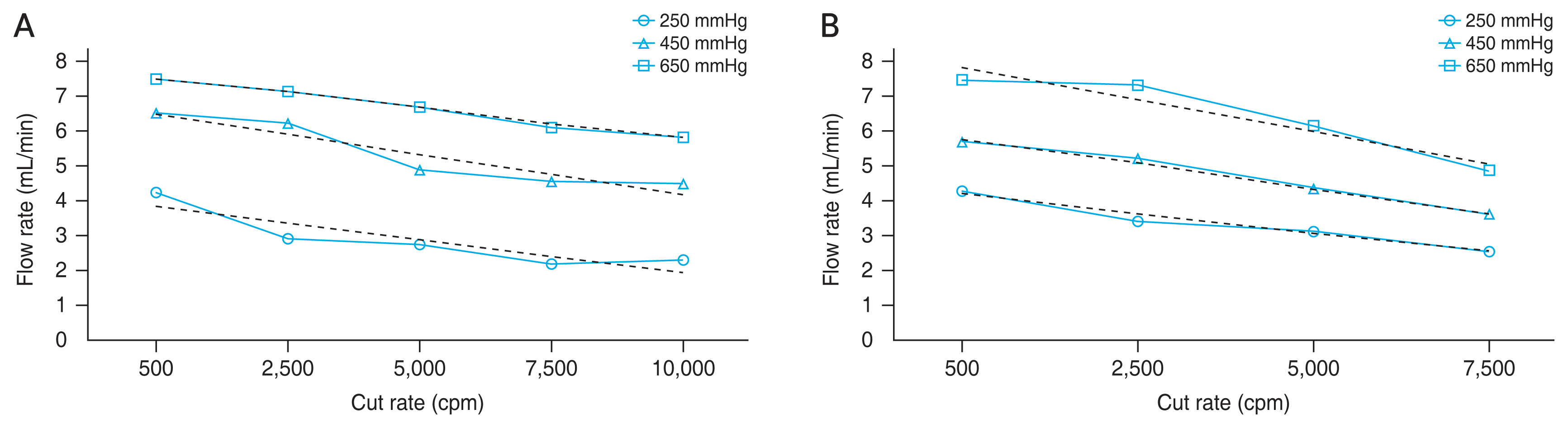
Egg white flow rates of 23-gauge vitreous cutters in biased open duty cycle. (A) Advanced UltraVit 10,000 cuts per minute (cpm) cutter. (B) UltraVit 7,500 cpm cutter. Each data point represents the average flow rate, and dashed lines indicate linear regression trends.
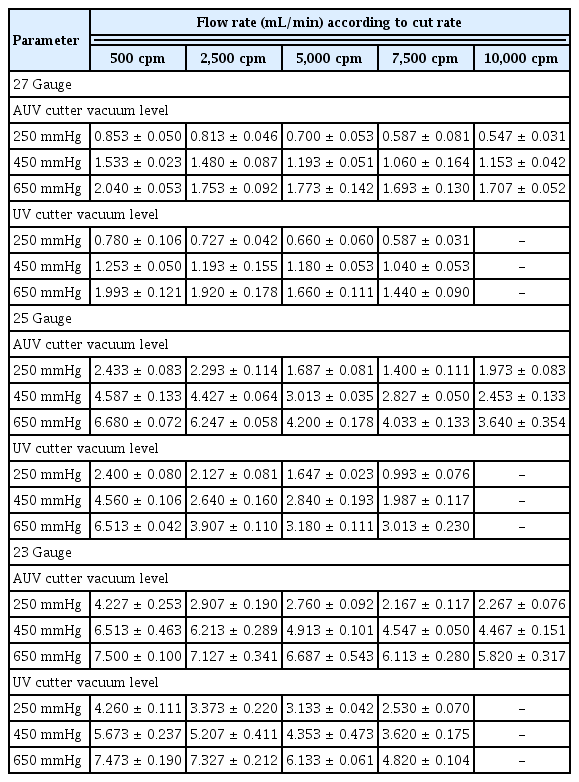
Flow rate under each parameter
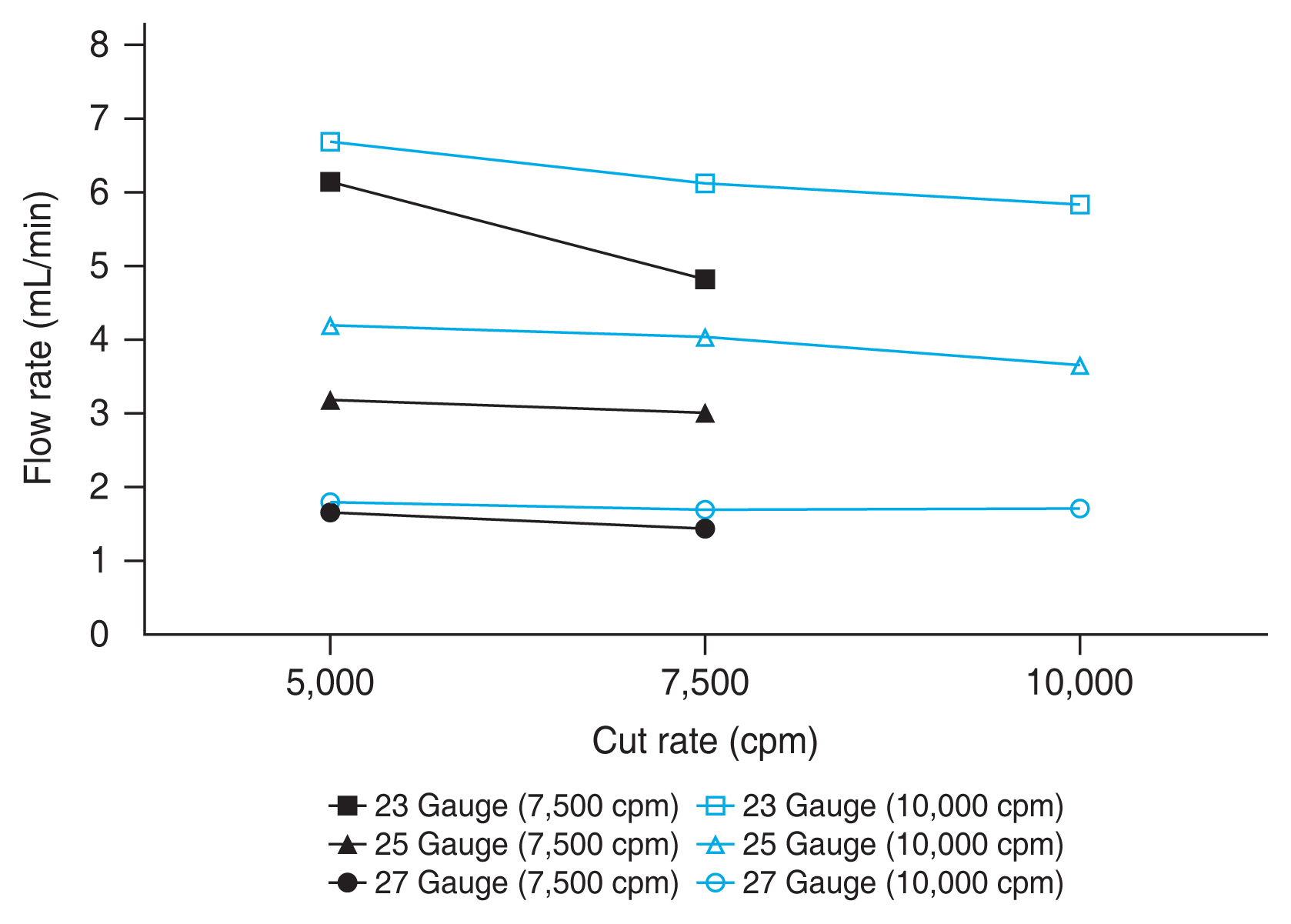
Egg white flow rates of vitreous cutters in biased open duty cycle under 650 mmHg vacuum. Each data point represents the average flow rate. cpm = cuts per minute.
For 27 gauge, with the 650-mmHg vacuum setting, the slopes of the linear trend line were found to be −0.029 μL/ cut (r2 = 0.657) with the AUV cutter and −0.077 μL/cut (r2 = 0.959) with the UV cutter. For 25 gauge, the slopes of the linear trend line were −0.332 μL/cut (r2 = 0.883) with the AUV cutter and −0.449 μL/cut (r2 = 0.800) with the UV cutter under the 650-mmHg vacuum setting. For 23 gauge, the slopes of the linear trend line were −0.175 μL/cut (r2 = 0.992) and −0.366 μL/cut (r2 = 0.916) at 650 mmHg vacuum pressure for the AUV and the UV cutters, respectively. For both AUV and UV cutters, the 27-gauge probe showed the lowest change in flow rate with increasing cut rates (p < 0.05).
The times required to remove 4 mL of egg white under the setting of the maximum cut rates and the maximum vacuum level in the biased open duty cycle using the AUV cutter were 149.07 ± 6.93 seconds for 27 gauge, 59.33 ± 3.51 seconds for 25 gauge, and 36.33 ± 3.21 seconds for 23 gauge. Under the same condition, the times required to remove 4 mL of egg white using the UV cutter were 169.33 ± 6.13 seconds for 27 gauge, 76.67 ± 5.03 seconds for 25 gauge, and 45.00 ± 2.65 seconds for 23 gauge. It took longer time to remove the same volume of egg white as the diameter of the vitreous cutter decreased. Further, among vitreous cutters with the same gauge, the UV cutter took longer than the AUV cutter, thus corresponding to the above experimental results (independent t-test, all p < 0.05) (Table 2).
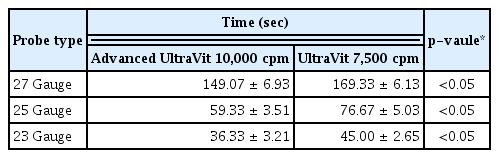
Time consumed for egg white 4 mL removal
Discussion
To ensure stability and minimize complications during vitrectomy, it is important to maintain equal fluid inflow and outflow. Several factors can affect outflow, including the viscosity of the aspirated fluid, the size of the fragmented vitreous, the inner diameter of the vitrectomy probe, the turbulence of the fluid in and around the vitrectomy probe, the structure of the vitrectomy probe, the size of the port, the length of the aspiration tube, the vacuum level, the cut rates, and the duty cycle [9–11]. The viscosity of the aspirated vitreous varies depending on the initial viscosity of the vitreous, changes in viscosity caused by the cutting action of the vitreous cutter, and the resistance of the fluid within the aspiration tube [12]. Unlike water, which is easily aspirated, vitreous needs to be cut into small pieces before it can be aspirated [6].
The AUV and UV vitreous cutters used in this study each have a single blade and operate via a dual pneumatic system. This study found that the maximum flow rates occurred at the lowest cut rates in the biased open duty cycle. The flow rates tended to decrease as the cut rates increased, and this trend was found to be consistent across all vitreous cutters used in this study and did not vary by diameter. Similar results were found in other studies using water or balanced salt solution, as water is a low-resistance liquid that can be easily aspirated without needing to be cut [6,8,12]. As the cut rate increases, the duty cycle decreases and the time the port is open is relatively reduced, thus resulting in a decrease in flow rate. Vitreous is a viscous material that can block the port of the vitreous cutter and increase the resistance inside the aspiration tube. As the cut rates increase, the vitreous is cut into smaller pieces, which reduces the resistance during aspiration, thus resulting in an increase or constant flow rate [6,7,12].
All vitreous cutters used in this study showed an increase in flow rate as the vacuum level increased. When the diameter of the vitreous cutter decreased, a stronger vacuum level was required to maintain a high flow rate to offset the pressure loss. At maximum vacuum level and maximum cut rates, with a smaller gauge vitreous cutter, the flow rate decreased and required longer time to remove the egg white. Under the same conditions, 23-, 25-, and 27-gauge vitreous cutters all showed higher flow rates with the AUV cutter than with the UV cutter (Fig. 4), and the time consumed to remove the egg white was shorter for the AUV cutter as well. This means that using the AUV cutter for vitrectomy surgery allows for faster removal of the vitreous in comparison to using the UV cutter at all cut rates. The port size was larger on the AUV cutter than on the UV cutter, approximately from 0.15 to 0.19 inches for 23 gauge, approximately from 0.15 to 0.16 inches for 25 gauge, and approximately from 0.13 to 0.14 inches for 27 gauge [13]. As the port size increased, the amount of fluid flowing in at once would have increased, which would have had a positive effect on the flow rate. Increasing the port size of a vitreous cutter is an effective way to increase flow rates until it reaches a critical diameter [14]. Additionally, duty cycle was improved in the AUV cutter compared to the UV cutter, which converged at approximately 60% as the cut rates increase in the AUV cutter while the UV cutter converged at 50% [13]. In our experiment, the flow rate of the AUV cutter was higher than that of the UV cutter when both were set to the same cut rates of 7,500 cpm. The reason why the AUV cutter shows higher flow rate than the UV cutter, even at the lower cut rate, would be multiple. Not only the difference of the maximum cutting speed, but also the difference in the port size and duty cycle might have affected the flow rate. These factors would have worked in combination.
One limitation of this study is that the experiments were performed in an open-sky setting without connecting the infusion cannula. In actual vitrectomy surgeries, the ratio of balanced salt solution and vitreous humor changes continually, which was not reflected in this experiment. Different diameters and cut rates result in differences in the time required to remove the same amount of egg white in experimental conditions. In actual vitrectomy surgeries, the time required for vitreous removal can also be affected by factors such as age of the patient, the degree of vitreous liquefaction, and the surgeon’s skill, as not only the vitreous but also the inflowing balanced salt solution is removed during vitrectomy. Therefore, if the diameter of the vitrectomy probe is small and the cut rate is high, and if the probe does not approach closely to the vitreous, then balanced salt solution may be aspirated more than the vitreous, therefore resulting in a longer operation time.
Furthermore, one of the substances similar to the vitreous, egg white, was selected and used for the experiment, but it should be noted that there may be differences in the composition, and it is necessary to be cautious when interpreting the results [15,16]. Further experiments and studies with animal vitreous like human vitreous may help overcome the limitations caused by differences in composition. Moreover, in this study, only the biased open duty cycle of the dual pneumatic vitreous cutter was used, indicating that there is a need for further research on the 50/50 and biased closed duty cycle.
In summary, vitrectomy is evolving, focusing on the miniaturization of the probe and the increase in the cut rates. Using a smaller gauge vitreous cutter may reduce the flow rate and increase the time required for vitrectomy, but this can be partially compensated for by increasing the vacuum level as well as using a vitreous cutter with a higher maximum cut rate, improved port size, and improved duty cycle. This study is expected to give a useful information about how the vitreous cutters should be developed as the probe diameter decreases. Although predicting the flow rate in actual surgery is more difficult due to the viscosity of the vitreous, this study would be helpful in not only selecting a vitreous cutter for effective surgery but also in understanding the future development of vitreous cutter systems.
Acknowledgements
None.
Notes
Conflicts of Interest: None.
Funding: This work was supported by the Soonchunhyang University Research Fund. The funder had no role in study design, decision to publish, or preparation of the manuscript.