Leukostasis Retinopathy as the First Sign of Chronic Myeloid Leukemia with Severe Hyperleukocytosis: Two Case Reports
Article information
Dear Editor,
Chronic myeloid leukemia (CML) is a myeloproliferative neoplasm resulting from BCR-ABL translocation [1]. Typical retinopathy caused by CML includes retinal hemorrhages, Roth spots, cotton wool spots, venous dilatation, and tortuosity due to the penetration of leukemic tumor cells or secondary influence through anemia and thrombocytopenia [2]. Leukostasis, also known as symptomatic hyperleukocytosis, forms plugs consisting of white blood cells with increased volume and adhesion, which cause microvascular occlusion. Leukostasis retinopathy is a rare complication of CML compared to typical leukemic retinopathy. Herein, we report retinal and choroidal changes in patients with leukostasis retinopathy as the first sign of CML using multimodal imaging. Informed consents for publication of the research details and clinical images were obtained from the patients.
A 19-year-old male patient without any underlying systemic disease was referred for blurry vision in both eyes for 4 days without any other symptoms. The initial best-corrected visual acuity (BCVA) was 20 / 50 in both eyes. Fundus examination in both eyes revealed dilated and tortuous retinal veins, multiple intraretinal hemorrhages, Roth spots, and white leukemic infiltrates (Fig. 1A). Optical coherence tomography (OCT) revealed severe subretinal fluid (SRF), intraretinal fluid (IRF), and multiple inner layer hyperreflectivity (Fig. 1B). Ultra-widefield fluorescein angiography (UWFA) revealed a peripheral nonperfusion area, diffuse microaneurysm, and mild retinal vessel leakage (Fig. 1C). However, UWF indocyanine green angiography (ICGA) did not reveal choroidal nonperfusion (Fig. 1D). OCT angiography (OCTA) revealed focal nonperfusion lesions and decreased vascular density (VD) in the superficial capillary plexus (SCP), deep capillary plexus (DCP), and choriocapillaris (CC) (Fig. 1E). Routine blood tests showed markedly elevated white blood cell (WBC) count (501,800/mm3). Bone marrow biopsy in the hemato-oncology department confirmed BCR/ABL translocation, leading to the diagnosis of CML. The patient was prescribed oral dasatinib (1,000 mg). After 7 months of dasatinib treatment, BCVA in both eyes improved to 20/25 and UWF and OCT findings also improved; however, the outer retinal disruption remained (Fig. 1F, 1G). The VD of the SCP and DCP in OCTA was partially improved, and the DCP showed a low recovery, far below the normal value of 57.87% [3]. The VD of the CC showed a relatively high recovery; however, the focal capillary dropout remained (Fig. 1H).
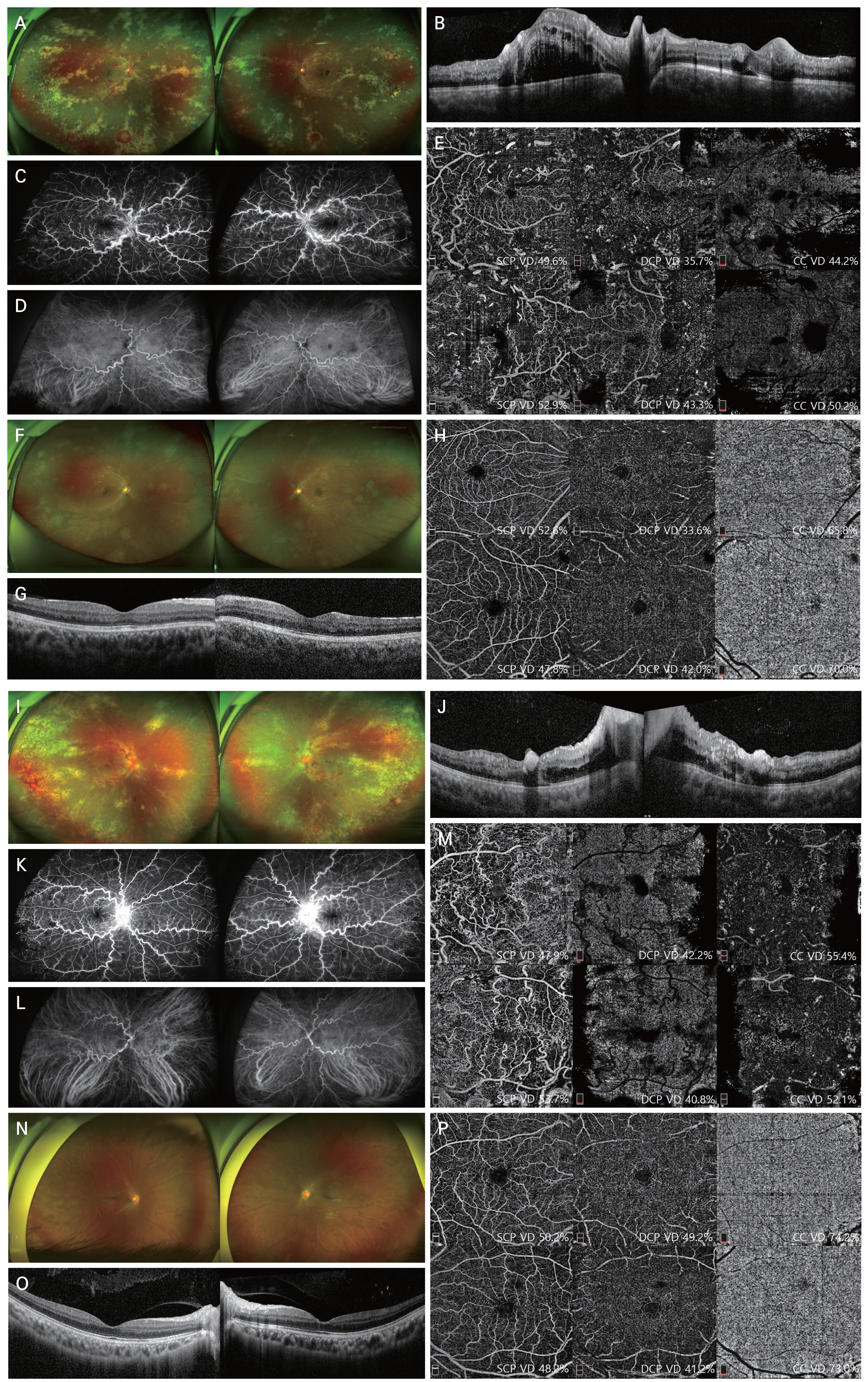
Images of the two cases. (A–H) Case of the 19-year-old male patient. (A–E) Initial images. (A) Ultra-widefield (UWF) retinal imaging in both eyes showed marked venous dilatation and tortuosity, multiple retinal and preretinal hemorrhages, Roth spots, and multiple whitish retinal infiltrates. (B) Optical coherence tomography (OCT) revealed subretinal fluid (SRF) and intraretinal fluid (IRF), thickened choroid and blot hyperreflective lesions in the inner retinal layer in both eyes. (C) UWF angiography (UWFA) showed hypofluorescence at the temporal area and diffuse leakage in both eyes. (D) UWF indocyanine green angiography (ICGA) showed no abnormalities other than dilatation of choroidal vessels. (E) Baseline OCT angiography (OCTA) of the superficial capillary plexus (SCP), deep capillary plexus (DCP), and choriocapillaris (CC) in the 6 × 6-mm area centered on the fovea. OCTA image showed blockage areas due to the screen effect from hemorrhage and focal nonperfusion lesions on the SCP, DCP, and CC in both eyes. The images of the upper line of the OCTA are the right eye, and the images of the lower line are the left eye. (F–H) Images after treatment. (F,G) After 7 months of treatment with dasatinib, UWF and OCT findings almost improved, but outer retinal disruption remained. (H) OCTA images of the SCP, DCP, and CC revealed focal nonperfusion lesion in both eyes. (I–P) Case of the 25-year-old male patient. (I–M) Initial images. (I) UWF retinal imaging in both eyes showed intraretinal hemorrhages, Roth spots, and venous tortuosity. Optic disc swelling was noted in both eyes. (J) OCT showed shallow SRF and IRF and hyperreflective lesions in the inner retinal layer in both eyes. (K) Initial UWFA demonstrated nonperfusion areas in the peripheral retina. Vascular and disc leakage was noted in both eyes. (L) Choroidal nonperfusion was not seen in either eye at baseline UWF ICGA. (M) Baseline OCTA of SCP, DCP, and CC showed blocked areas and nonperfusion lesions. (N–P) Images after treatment. (N,O) After 8 months of treatment with dasatinib, UWF and OCT imaging improved over initial images. (P) OCTA images showed slight improvement in vessel density of SCP, DCP and CC compared to the initial but focal capillary dropout remained. VD = vascular density.
A 25-year-old male patient with no previous medical history was referred for rapid visual loss in both the eyes for 1 day. The initial BCVA was 20 / 125 and 20 / 2,000 in the right and left eyes, respectively. Fundus examination showed clinical features similar to the previous case, accompanied by optic disc edema in both eyes (Fig. 1I). OCT revealed shallow SRF, IRF, and hyperreflective lesions in the inner retinal layer in both eyes (Fig. 1J). The UWFA, UWF ICGA, and OCTA findings were similar to those of the previous case (Fig. 1K–1M). CBC confirmed a WBC count of 482,180/mm3. The patient received the same treatment for 8 months, with the same diagnosis as the previous patient. BCVA improved to 20 / 20 and 20 / 25 in the right and left eyes, respectively, and the fundus findings also improved (Fig. 1N, 1O). The VD changes of the SCP, DCP, and CC in OCTA were similar to those of the previous case (Fig. 1P).
Specifically, this report is unique in that it describes the pathological changes in leukostasis retinopathy on multimodal imaging in a follow-up of approximately 8 months. In the UWFA and OCTA of our cases, the focal nonperfusion area was mainly observed in the periphery rather than the macula. As peripheral retinal vessels require high perfusion pressure to pump blood, they are more sensitive to small changes in the blood flow and show more severe ischemic changes than the macula [4]. After systemic treatment, foveal microvascular abnormalities remained in the macular area on OCTA. These cases suggest that partial ischemia of the retinal capillaries may persist even after remission of CML. The VD of the CC in OCTA recovers close to normal values with the help of abundant choroidal blood flow, but not sufficiently in SCP and especially in DCP. The DCP has an interlocking meshwork of similar capillary-sized vessels and is vertically connected to the SCP without collateral channels, resulting in decreased perfusion of the DCP [5]. Overall, early diagnosis of leukostasis retinopathy through multimodal imaging, prompt referral to hemato-oncology, and continuing ophthalmic examinations after hematological remission are important.
Acknowledgements
None.
Notes
Conflicts of Interest: None.
Funding: None.