Comparison of Each Retinal Layer Thicknesses between Eyes with Central Retinal Vein Occlusion and Normal Contralateral Eyes
Article information
Abstract
Purpose
To evaluate the difference in each retinal layer thickness in central retinal vein occlusion (CRVO) with resolved macular edema after intravitreal antivascular endothelial growth factor injection and normal contralateral eyes..
Methods
Patients with ischemic and nonischemic CRVO whose macular edema resolved after intravitreal antivascular endothelial growth factor injections and did not recur for at least 6 months, and a normal contralateral eye were enrolled. Each retinal layer thickness between CRVO and normal contralateral eyes was compared according to Early Treatment Diabetic Retinopathy Study subfields using spectral domain optical coherence tomography.
Results
The thicknesses of outer nuclear layer, photoreceptor layer, and retinal pigment epithelium in central ring, ganglion cell layer, inner plexiform layer, outer nuclear layer, and photoreceptor layer in the inner ring, and ganglion cell layer in the outer ring of CRVO eyes were significantly thinner than those of normal contralateral eyes (all p < 0.05). Whereas, inner nuclear layer and outer plexiform layer thicknesses in central ring of CRVO eyes were 23.86 ± 8.8 and 25.76 ± 7.6 μm, respectively, which was significantly thicker than those of normal contralateral eyes (19.52 ± 7.7 and 22.76 ± 6.5 μm; p = 0.019 and p = 0.043, respectively). Additionally, the mean best-corrected visual acuity of CRVO eyes were significantly correlated with photoreceptor layer thickness in central ring (p = 0.005).
Conclusions
In CRVO eyes with resolved macular edema, the outer retinal layers were thinner as well as inner retinal layers, whereas inner plexiform layer and outer nuclear layer were thicker than normal fellow eyes. Additionally, photoreceptor layer thickness in foveal area had a significant impact on visual acuity in CRVO.
Central retinal vein occlusion (CRVO) happens when a blood clot blocks the flow of blood through the retina’s main vein [1]. It causes macular edema (ME) and subsequent vision loss and is common in people with diseases such as arteriosclerosis, diabetes, and hypertension [2,3]. The prevalence was 0.1% to 0.4% and about 2.5 million people worldwide are being influenced [3,4]. Nonischemic CRVO, called “venous stasis retinopathy” is more common than the ischemic form which characterized by substantially decreased retinal perfusion with capillary closure and retinal hypoxia. Ischemic CRVO, defined as a case of 10 disc diameters or more nonperfusion area in fundus fluorescent angiography, is a more severe form leading to worse prognosis compared to nonischemic form [3,5,6]. Both forms of CRVO can cause ME and neovascularization, and various treatments for CRVO-associated ME have been trialed, including intravitreal antivascular endothelial growth factor (anti-VEGF) injection and laser photocoagulation [7].
Optical coherence tomography (OCT) is a noninvasive diagnostic tool, which provides cross-sectional retinal images with fine resolution, including microstructural retinal layer measurement [8]. Using spectral domain OCT (SD-OCT), Podkowinski et al. [9] reported that 12.6% of the CRVO eyes and 10.3% of the branch retinal vein occlusion (BRVO) eyes with resolved ME showed the thinning of inner retinal thicknesses in focal macular area after ranibizumab therapy. Kim et al. [10] revealed that ganglion cell-inner plexiform layer (GCIPL) thickness is thinner in eyes with resolved macular edema in CRVO than non-ME CRVO eyes by using SD-OCT. However, few studies that evaluated each retinal layer thickness including outer retina have been reported [9,10].
In this study, we evaluated differences in each retinal layer thickness of CRVO eyes with resolved ME and normal contralateral eyes. Also, we evaluated the correlation between each retinal layer and visual acuity.
Materials and Methods
Ethics statement
This study was in compliance of Declaration of Helsinki and was registered by the Institutional Review Board of Konyang University Hospital, Daejeon, Korea (No. 2021-11-003). The requirement for informed consent was waived due to the retrospective nature of the study.
Patients
We retrospectively reviewed the charts of 31 patients diagnosed with ischemic and nonischemic CRVO at Konyang University Hospital between June 2017 and June 2021. Patients with CRVO whose ME resolved after intravitreal anti-VEGF injections and did not recur for at least 6 months, and with normal contralateral eye were enrolled. Ophthalmic examinations included best-corrected visual acuity (BCVA) using Snellen visual acuity chart converted to logarithm of the minimum angle of resolution, intraocular pressure (IOP) using noncontact tonometry, and spherical equivalent. The exclusion criteria were as follows: IOP ≥21 mmHg; BCVA <20 / 400 after resolved ME; any ophthalmic disease that could affect the retinal layer thickness such as glaucoma, retinal, and neuro-ophthalmic diseases except CRVO; and a history of intraocular surgery except cataract extraction. Patients who received laser photocoagulation which could cause retinal atrophy were also excluded.
OCT measurements
Retinal layer thickness was obtained by an experienced examiner using SD-OCT (Spectralis; Heidelberg Engineering, Heidelberg, Germany). Each layer thickness measurement from SD-OCT were conducted by Spectralis built-in segmentation systems, Heidelberg Eye Explorer ver. 6.9a (Heidelberg Engineering). The central, inner, and outer rings were divided based on the nine subfields of Early Treatment Diabetic Retinopathy Study, which was 1 mm central, 1 to 3 mm, and 3 to 6 mm (outer section of the inner ring), respectively (Fig. 1). The retinal layer thickness of inner and outer rings was calculated by averaging four values of superior, nasal, inferior, and temporal segments of 1 to 3 mm and 3 to 6 mm each. Segmented layers, including retinal nerve fiber layer (RNFL), ganglion cell layer (GCL), inner plexiform layer (IPL), inner nuclear layer (INL), outer plexiform layer (OPL), outer nuclear layer (ONL), photoreceptor layer (PRL), and retinal pigment epithelium (RPE), were measured. PRL thickness was measured by substracting RPE thickness from outer retinal layers thickness. Full retinal thickness (FRT) was also obtained. Manual adjustment was performed when obvious segmentation error was found. All scans that had any motion artifact, misalignment, segmentation system failure, incomplete image taking, or low resolution were excluded.
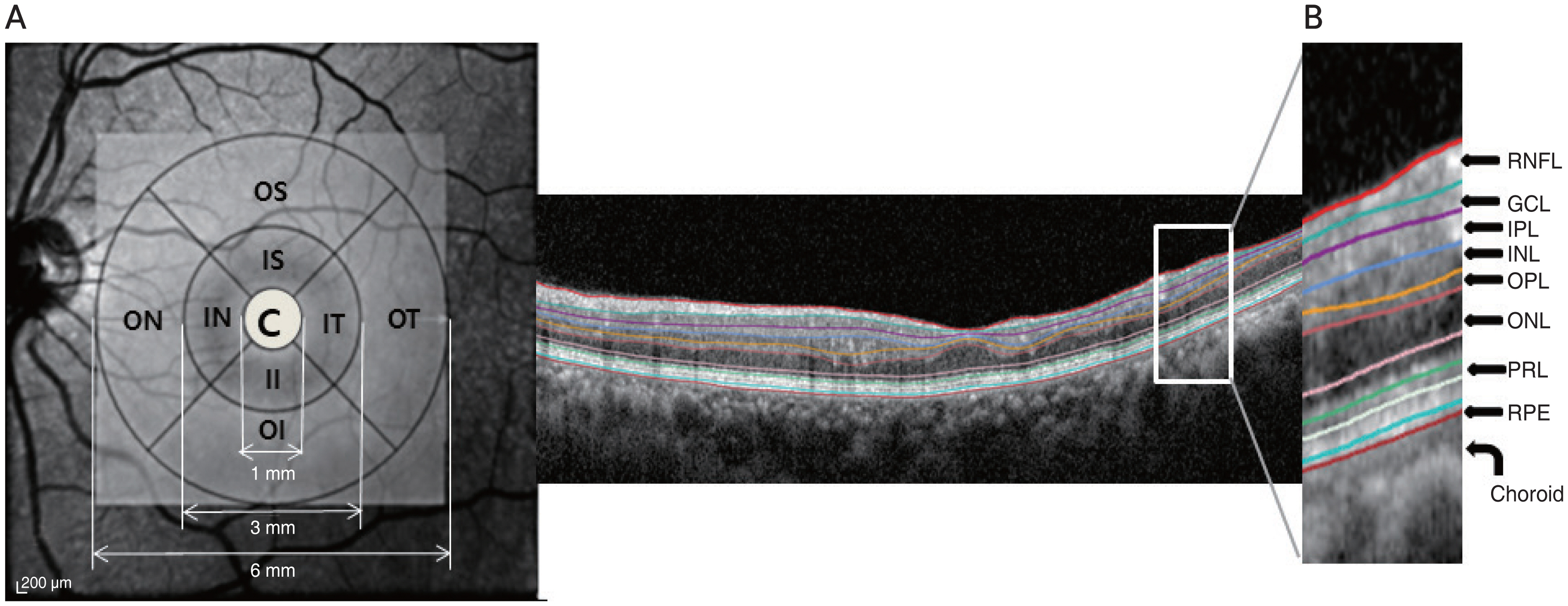
Macular regions analyzed by spectral domain optical coherence tomography scan in the retinal thickness map analysis. (A) The macular was divided into three subfields: the central ring (C) with the diameter of 1 mm, the inner ring ranging from 1 to 3 mm from the central ring, and the outer ring from 3 to 6 mm from the central ring. Retinal layer thickness of inner and outer rings was calculated by averaging four values of superior, nasal, inferior, and temporal segments of 1 to 3 mm and 3 to 6 mm each. (B) The boundaries of fundus structure were segmented by an automated algorithm, and the thickness profiles of the each retinal sublayers and choroid were determined. IS = inner superior; IN = inner nasal; II = inner inferior; IT = inner temporal; OS = outer superior; ON = outer nasal; OI = outer inferior; OT = outer temporal; RNFL = retinal nerve fiber layer; GCL = ganglion cell layer; IPL = inner plexiform layer; INL = inner nuclear layer; OPL = outer plexiform layer; ONL = outer nuclear layer; PRL = photoreceptor layer; RPE = retinal pigment epithelium.
Statistical analysis
Ophthalmic examinations between CRVO eyes and normal fellow eyes were compared by using paired t-test. Pearson correlation was performed to identify the relationship between BCVA and each retinal layer thickness. Data was analyzed by using IBM SPSS ver. 20.0 (IBM Corp., Armonk, NY, USA).
Results
Demographics
A total of 62 eyes of 31 participants were enrolled: 31 eyes with CRVO and 31 normal contralateral eyes. The mean participants age was 60.0 ± 14.6 years (Table 1). There were 16 male patients (51.6%). The mean follow-up duration was 2.8 ± 2.2 years, and recurrence-free period after resolved ME was 9.9 ± 7.0 months. The mean BCVA (logarithm of the minimum angle of resolution) was significantly different between CRVO eyes and controls, showing 0.62 ± 1.0 and 0.05 ± 0.1 (p = 0.003). The mean spherical equivalent and IOP were −0.25 ± 1.4 and 14.14 ± 3.4 mmHg, respectively, in CRVO eyes and −0.31 ± 1.8 and 13.97 ± 3.4 mmHg, respectively, in controls, which were not significantly different (p = 0.742 and p = 0.784, respectively). The mean number of bevacizumab injections in CRVO eyes was 8.24 ± 6.7. Intravitreal triamcinolone injection was performed in two patients.

Demographics and characteristics of patients (n = 31)
OCT measurements
1) Quantitative analysis of central ring
The mean thickness of each retinal layer in the central ring is shown in Table 2. The average thicknesses of ONL (78.79 ± 20.7 μm vs. 90.07 ± 14.1 μm, p = 0.001), PRL (70.10 ± 4.1 μm vs. 71.90 ± 3.7 μm, p = 0.012), and RPE (15.38 ± 1.6 μm vs. 16.24 ± 2.7 μm, p = 0.013) were significantly different between CRVO eyes and normal fellow eyes; CRVO eyes were thinner than normal eyes. However, the thickness of INL and OPL was 23.86 ± 8.8 and 25.76 ± 7.6 μm in CRVO eyes, respectively, which was thicker than that of fellow eyes (19.52 ± 7.7 and 22.76 ± 6.5 μm; p = 0.019 and p = 0.043, respectively). There were no significant differences in FRT, RNFL, GCL and IPL between the two groups.
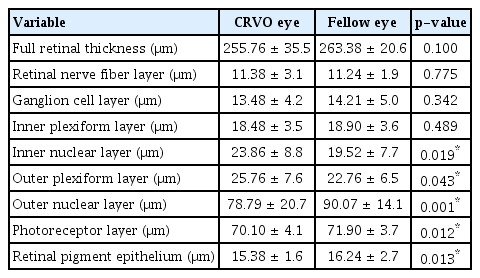
Comparison of retinal layer thickness in the central field of the ETDRS grid in the eyes resolved macular edema by CRVO and the fellow eyes
2) Quantitative analysis of inner ring
FRT was significantly thinner in CRVO eyes than fellow eyes (313.64 ± 42.5 μm vs. 329.89 ± 20.2 μm, respectively; p = 0.024) (Table 3). Additionally, each thickness of GCL, IPL, ONL, and PRL was thinner in CRVO eyes than those in fellow eyes; the average GCL thickness was 40.43 ± 13.3 μm in CRVO eyes and 46.50 ± 7.5 μm in fellow eyes (p = 0.011), the average IPL thickness was 34.86 ± 8.7 μm in CRVO eyes and 38.46 ± 4.4 μm in fellow eyes (p = 0.015), the average ONL thickness was 64.74 ± 3.5 μm in CRVO eyes and 68.38 ± 8.6 μm in fellow eyes (p = 0.044), and the average PRL thickness was 65.80 ± 1.9 μm in CRVO eyes and 66.10 ± 1.9 μm in fellow eyes (p < 0.001).

Comparison of retinal layer thickness in the inner ring of the ETDRS grid in the eyes resolved macular edema by CRVO and the fellow eyes
3) Quantitative analysis of outer ring
There were no statistically significant differences in most of the layers except GCL (Table 4). The average thickness of GCL was 30.24 ± 8.1 μm in CRVO eyes, which was significantly thinner than 33.83 ± 4.8 μm in fellow eyes (p = 0.024).

Comparison of retinal layer thickness in the outer ring of the ETDRS grid in the eyes resolved macular edema by CRVO and the fellow eyes
4) Correlation analyses with the thickness of each retinal layer and visual acuity
The PRL thickness of foveal area was significantly correlated with BCVA (r = −0.503, p = 0.005). Other retinal layers, including RNFL (r = −0.082, p = 0.673), GCL (r = 0.030, p = 0.875), IPL (r = −0.085, p = 0.662), INL (r = 0.169, p = 0.381), OPL (r = 0.032, p = 0.867), OPL (r = 0.054, p = 0.779), ONL (r = −0.307, p = 0.106), and RPE (r = −0.216, p = 0.260) did not show the significant result.
Discussion
We analyzed the each retinal layer of CRVO eyes and normal fellow eyes and found that the ONL, PRL, and RPE of CRVO eyes were thinner than those of the fellow eyes in the central part, whereas the INL and OPL were thicker. In the inner ring, GCL, IPL, ONL, and PRL of the CRVO eyes were thinner than those of fellow eyes. In the outer ring, GCL of the CRVO eyes was thinner than those of the fellow eyes. Additionally, the central thickness of PRL showed a significant correlation with BCVA in CRVO eyes.
Kim et al. [10] reported that the minimum thickness of GCIPL in CRVO eyes with resolved ME after intravitreal anti-VEGF injection was significantly thinner than that of GCIPL in CRVO eyes without ME (54.07 ± 22.17 μm vs. 66.83 ± 19.88 μm, p = 0.022). Podkowinski et al. [9] reported the retinal thinning of the inner retinal compartment in focal macular areas in 11% of retinal vein occlusion (RVO) eyes with resolved ME after ranibizumab therapy. As in previous studies, the GCL and IPL thickness of CRVO eyes were thinner than those of fellow healthy eyes in this study. Under hypoxia in the CRVO retina, the levels of VEGF, nitric oxide, free oxygen radicals, glutamate, and inflammatory cytokines increased, which could lead to cell death of retinal ganglion cells [11,12]. Decreased vascular density in RVO eyes, which is related to inner retinal thickness, is also possibly associated with inner retina reduction [13–16]. Additionally, anti-VEGF treatment can damage the ganglion cells and disturb autocrine VEGF-induced retinal ganglion cells survival [17,18]. Long-term suppression of neurotrophic cytokines can damage to GCL to RNFL and cause inner retinal thinning during chronic anti-VEGF treatment [19–21].
This study found that INL and OPL thicknesses in the CRVO eyes were significantly thicker than normal fellow eyes, especially in the foveal area. Joltikov et al. [22] reported that INL + OPL were significantly thicker in patients with nonprogressive diabetic retinopathy compared to healthy controls. Yamada et al. [23] also reported an increase in INL and OPL in patients with diabetic polyneuropathy compared with normal controls. They explained that these increases were related to the reactive gliosis of Muller cells in the INL. In a previous study, electron microscopic findings verified reactive gliosis, which is a progressive transformation from the Muller cell phenotype to a poorly differentiated glial cell phenotype and the proliferation of glial cell processes in patients with diabetes [24]. Although the exact mechanism is unknown, the thickening of INL and OPL in eyes with CRVO may be related to Muller cell damages, which is similar to diabetes. Further histopathologic studies are needed in the future.
The mean thickness of PRL and RPE was thinner in the CRVO eyes than in the control group. Many previous studies have demonstrated that cardiovascular diseases such as hypertension and diabetes are highly correlated with CRVO [25–30]. Of the 31 participants in this study, 12 had hypertension, and 13 had diabetes mellitus. Patients with hypertension and diabetes mellitus have poor choroidal circulation. Geraci et al. [31] reported that oxidative stress and endothelial dysfunction, which are commonly found in early complications of hypertension, could lead to changes in vascular elastic properties and structural modification of the choroidal layer. In a population of 160 subjects (80 hypertensive subjects and 80 healthy control subjects), Akay et al. [32] demonstrated that choroidal thickness decreased in patients with systemic arterial hypertension. Kase et al. [33] reported that choroidal thickness and vasculature decreased in diabetes patients. Therefore, the dependence of the blood supply of outer retina would be high on the inner retinal layer in eyes with CRVO. Tsai et al. [13] reported that microvascular parameters revealed by OCT angiography in the RVO eyes decreased. Kim et al. [34] reported that superficial vessel density in RVO decreased, which could be explained by an enlarged foveal avascular zone area in OCT angiography. Therefore, whereas the contralateral eyes may have only choroidal circulation insufficiency, the CRVO eyes would be accompanied by choroidal circulation insufficiency as well as inner retina perfusion impairment. Therefore, since blood flow in both the choroid and inner retinal layers supplying perfusion to the outer retina decreases, the thinning of the outer retina would be caused by poor blood circulation in the outer retina in CRVO.
Kim et al. [10] reported that minimum GCIPL thicknesses was significantly correlated with BCVA in CRVO eyes with resolved ME after intravitreal anti-VEGF injections. Moreover, they reported that the thinner the minimum GCIPL thicknesses, the worse the BCVA. The importance of inner retinal layer thickness as a prognostic factor was also reported in other disease such as diabetic macular edema [35]. However, in our study, the other layers were not meaningful, and only the PRL in the central ring was associated with BCVA. Kang et al. [36] reported that intact inner/outer segment integrity of PRL and external limiting membrane status at baseline showed statistically significant correlation with better BCVA after intravitreal bevacizumab injection in ME secondary to BRVO. Shin et al. [37] found that the integrity of the foveal photoreceptor layer inner/outer segment are significantly correlated with final visual acuity in patients with resolved ME due to BRVO, and the smaller length of disrupted inner/outer segment of the foveal PRL on SD-OCT at initial visit is an indicators of better visual outcome in patients with RVO. Therefore, although the outer retina is also affected by inner retinal damage, the layer which is most directly related to ultimate visual acuity would be PRL.
There are some limitations in our study. First, the retrospective nature of this study inevitably introduces selection bias. Second, because of the limited follow-up duration, studies including patients with long-term follow-up period would be helpful in the future. Third, this study has small sample size, and the data was obtained from a single-center population, which may have the limitation of generalization of our study results. Fourth, this study did not have a normal control group. Therefore, it will be a meaningful study to compare it with a control group in the future. Additionally, although there was a significant difference of PRL and RPE thicknesses between CRVO eyes and normal contralateral eyes, the differences were relatively small. Further studies for repeatability for outer retinal layer thickness including PRL and RPE are needed in the future to increase the credibility of our paper. Despite the limitations, the strength of our study was that, to the best of our knowledge, this is the first study to identify each retinal layer thickness changes including outer retina in patients with CRVO with resolved ME.
In conclusion, we confirmed that the thicknesses of outer retinal layers including PRL and RPE became thinner as well as inner retinal layers in patients with CRVO with resolved ME than in controls; whereas INL and OPL in the foveal center became thicker in the diseasesed eyes than in normal fellow eyes. We also confirmed that thickness of PRL in the foveal area was significantly correlated with BCVA. These results suggest that CRVO-induced retinal ischemia caused changes in each retinal layer thickness, and the thickness of PRL would be the most important factor for visual prognosis in CRVO.
Acknowledgements
None.
Notes
Conflicts of Interest: None.
Funding: None.