Incidental Magnetic Resonance Imaging Findings of Postoperative Ocular Hypotony with Choroidal Effusion after Ahmed Glaucoma Valve Implantation: A Case Report
Article information
Dear Editor,
Postoperative hypotony after tube-shunt surgeries is known as common, yet sight-threatening complication. In ordinary ophthalmology clinics, it is evaluated with optical coherence tomography (OCT) or wide-field fundoscopy images, which can only provide information on axial plane. On the other hand, magnetic resonance imaging (MRI) can provide information on overall ocular structure, thus being used as an important imaging tool in many realms of ophthalmology [1,2]. With advances in perfusion MRI techniques, evaluation of ocular blood flow has been made possible as well [3].
Based on our literature review, a few reports describe MRI findings of eyes with hypotony due to causes other than glaucoma surgery. Commonly reported findings include overall thickening of sclera and flattening of posterior sclera, which was also observed in other OCT based studies. However, MRI images of postoperative hypotony and perfusion MRI images of such eventuality has not yet been reported.
Here, we report rare MRI finding of hypotonic eye with choroidal effusion, in which eccentric deformation of eyeball and perfusion changes were incidentally observed. A 15-year-old boy with uncontrolled intraocular pressure (IOP) was referred to the glaucoma clinic. Previously, he had already underwent two trabeculectomies on 2018 and 2019, and was using Monoprost (Thea, Clermont-Ferrand, France) and Cosopt-S (Santen Oy, Tampere, Filand) on his right eye. He presented with IOP of 45 mmHg in right eye, accompanied by pain. Corrected visual acuity was 0.02 and 1.0 (right and left, respectively), with slightly higher myopic error in the right. Anterior segment was clear with deep chamber and open angle. Corneal diameter and axial length of affected eye was longer than fellow eye (13.0/12.0 mm, 27.68/24.98 mm, respectively). Under the impression of late-onset primary congenital glaucoma, adult FP7 model of Ahmed glaucoma drainage device was implanted.
Five days after surgery, the patient showed good postoperative progress except hypotony; his IOP was 3 mmHg with choroidal detachment with no signs of papilledema. Despite significant ocular pain relief, brain MRI was performed at the request of his guardian due to his complaint of severe headache.
MRI was performed with standard contrast enhanced brain and neck MRI protocol with angiography. No neurological problems were detected. On T2-weighted and T2-weighted fluid-attenuated inversion recovery (FLAIR) image, well-positioned Ahmed glaucoma valve (AGV) was observed. Axial length was significantly shorter in the operated eye (23.01/24.69 mm), measured from apex of cornea to posterior sclera on transverse T1-weighted image. Interestingly, on sagittal and coronal T1-weighted images, inhomogeneous shrinkage of entire globe, ultimately forming a polygonal morphology with more prominent indentation near AGV (Fig. 1). Akagi et al. [4] reported morphological changes in highly myopic eyes after trabeculectomy, and reported that deformed regions of highly myopic eyes such as area of posterior staphyloma are more prone to morphological changes due to IOP reduction. Hence, decreased scleral rigidity due to buphthalmos and intrinsic weight of scleral fixated AGV may be attributable to the ocular deformity.
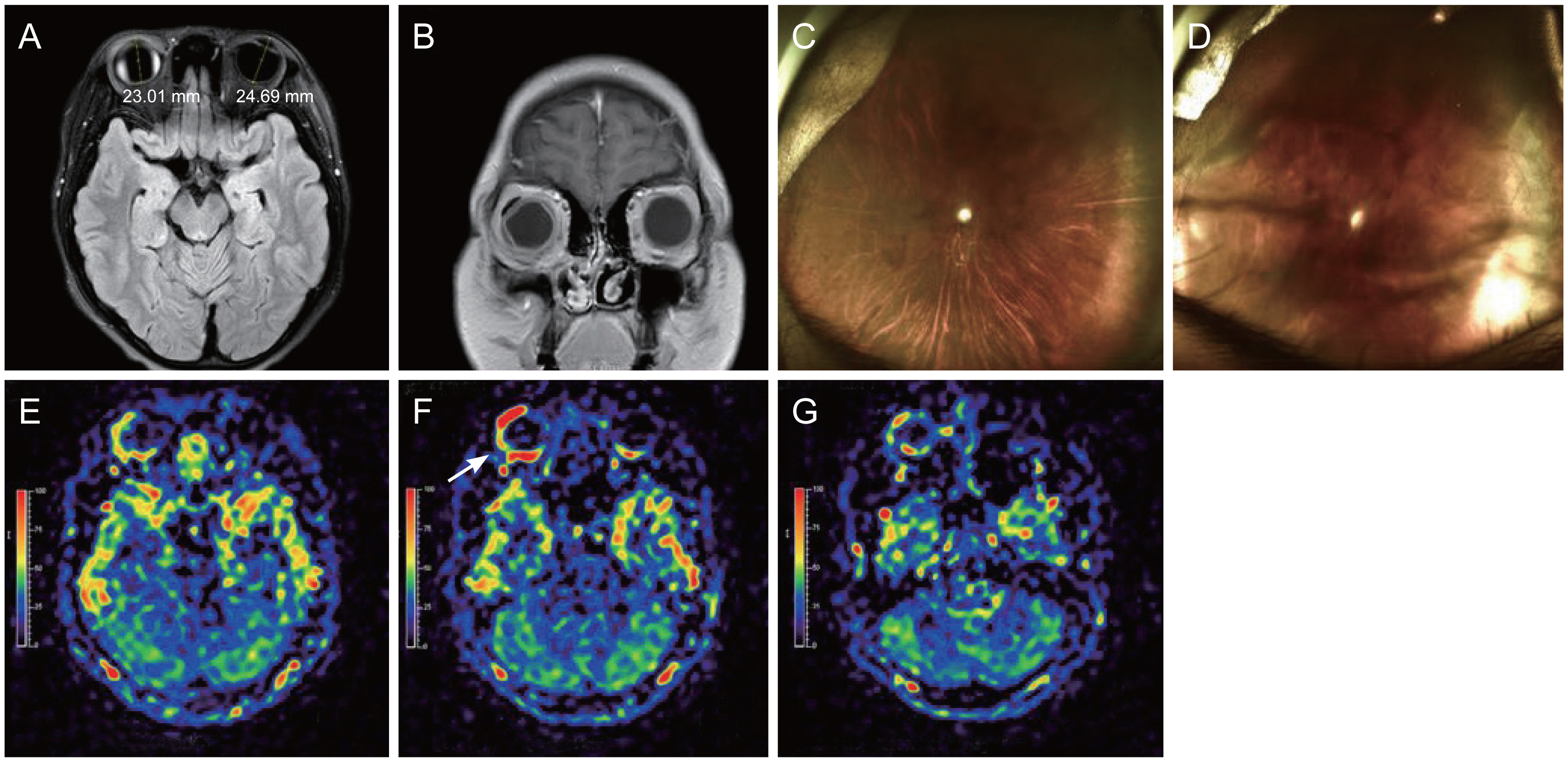
T2-weighted magnetic resonance imaging of an eye with postoperative hypotony and choroidal effusion. (A,B) Shortened axial length and irregularly shaped globe with prominent scleral depression along glaucoma drainage device is noticeable. Fundus photography (C) before surgery and (D) after surgery, showing peripheral choroidal detachments, but no signs of papilledema or hemorrhagic choroidal effusions. (E–G) Sequentially aligned pseudocontinuous arterial spin labelling images show increased perfusion (arrow), topographically distributed along glaucoma drainage device. Informed consent for publication of the clinical images was obtained from the patient’s guardian.
Another intriguing finding was from perfusion images, obtained by arterial spin labelling (ASL) MRI at 3.0 T using pseudocontinuous ASL labelling scheme. It was previously reported that chorioretinal blood perfusion can be quantitatively measured by using ASL-MRI with good reliability [3]. In our case, markedly increased perfusion signals circumambiently extending from temporal to posterior part of the globe, along AGV implant, was observed. At the very same area, scleral thickening with high signal intensity was noted on transverse FLAIR image. Whether this perfusion signal represent actual perfusion changes is not clear. However, making interpretations with previous reports, it may reflect inflammatory surge near AGV implantation site, which can be explained as either normal postoperative inflammation or a result of pathophysiologic process following hypotony [5]. Moreover, considering the abovementioned mechanical effect and coinciding area of perfusion and AGV implant, it can further be assumed that hydrostatic effect of mechanical compression of AGV may have contributed to the process. Interestingly, signs of choroidal effusion lasted longer than restoration of anterior chamber.
Considering paucity of our knowledge on the three-dimensional ocular morphologics and perfusion changes in low-toned eye, it provides rare information on ocular hypotony with choroidal effusion. The implications underlying these findings should further be discussed, but it can be of significant value in understanding of postoperative complications pertaining to glaucoma tube-shunt operations and it can also serve as an atlas for possible future researches.
Acknowledgements
None.
Notes
Conflicts of Interest: None.
Funding: This research was supported by a grant of the Medical data-driven hospital support project through the Korea Health Information Service (KHIS), funded by the Ministry of Health and Welfare, Korea.