


Dear Editor,
Retrobulbar anesthesia is a common anesthetic procedure for ophthalmic surgery. Complications of the procedure ranging from the relatively commonly encountered retrobulbar hemorrhage to life-threatening respiratory arrest have been reported [1]. Ocular penetration/perforation can occur as a rare complication with a poor prognosis. Importantly, choroidal neovascularization (CNV) can occur as an unusual late complication of ocular penetration/perforation during retrobulbar anesthesia [2]. Herein, we report a case that underwent intravitreal injection of bevacizumab for the treatment of macular CNV as a late sequela of retrobulbar anesthesia-related globe perforation.
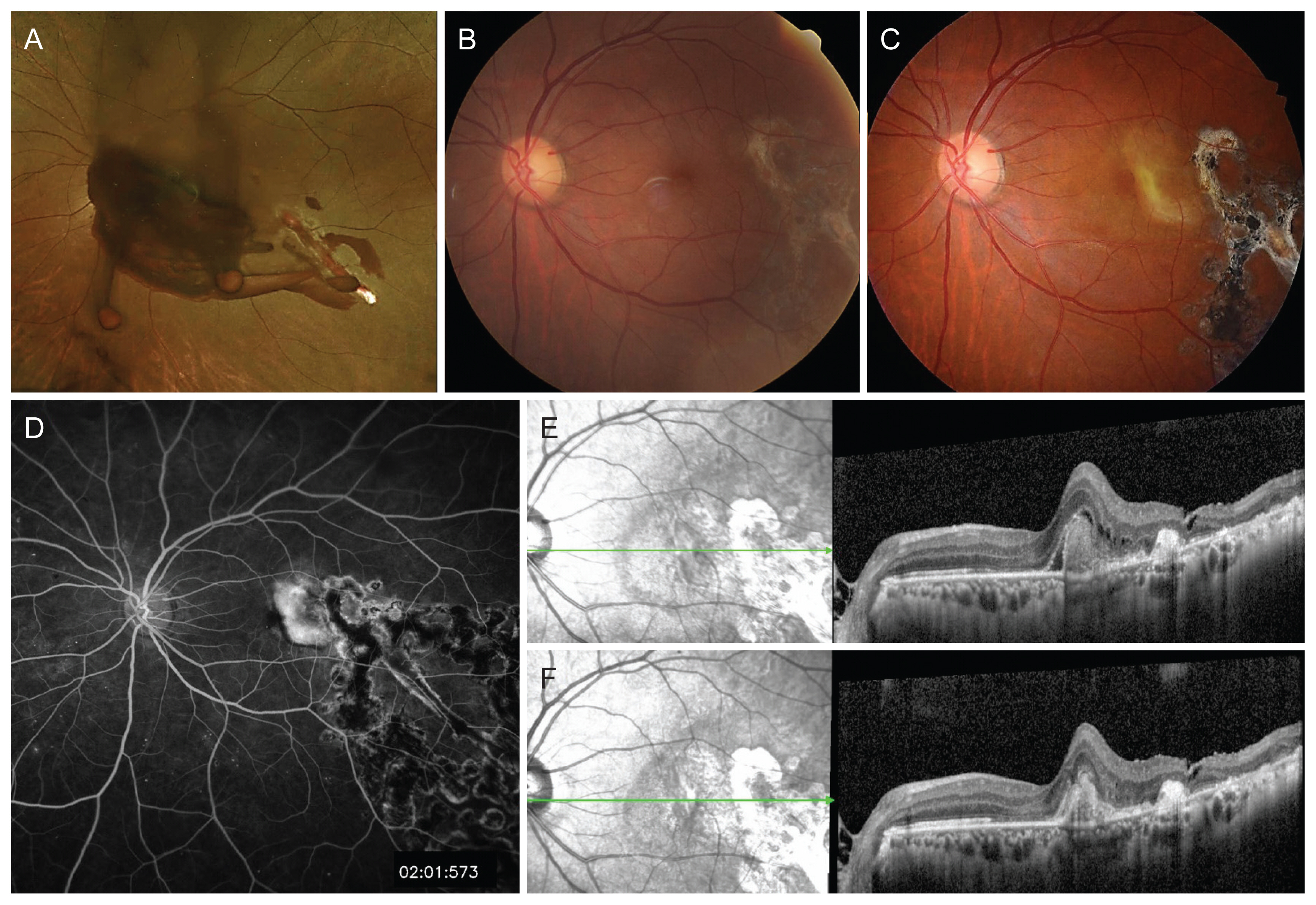
A 53-year-old male patient was referred to our clinic with a diagnosis of globe penetration during retrobulbar anesthesia for cataract surgery in the left eye. He had diabetes, hypertension, and hyperlipidemia, but no ocular medical history other than cataract. The axial length was 25.55 mm in the right eye and 25.34 mm in the left eye. The uncorrected visual acuity was 20/16 in the right eye using Snellen lines and hand motion in the left eye. Intraocular pressure was 13 mmHg in the right eye and 20 mmHg in the left eye. Anterior segment examination revealed no abnormalities. Fundus examination revealed vitreous hemorrhage and two penetrating wounds in the left eye (Fig. 1A). The patient underwent pars plana vitrectomy, vitreous hemorrhage removal, endolaser, and gas (18% SF6) tamponade. Two retinal holes were observed along the inferotemporal vascular arcade and approximately 2.5-disc diameters temporal to the fovea. Endolaser was performed around the retinal holes to prevent postoperative retinal detachment. On the fifth postoperative day, the visual acuity was 20/20 in the left eye using Snellen lines. Intraocular pressure was 8 mmHg in the left eye. After 2 weeks, fundus photography revealed retinal scarring without CNV (Fig. 1B). Thereafter, the patient was referred to a nearby hospital for regular checkup. After 1 year, the patient was referred again with decreased visual acuity in the left eye. The best-corrected visual acuity was 20/60 in the left eye. Fundus photography, optical coherence tomography, and fluorescein angiography revealed subfoveal CNV with subretinal fluid in the left eye (Fig. 1C-1E). For the treatment of CNV, he received three intravitreal injections of bevacizumab (Avastin; Genentech, South San Francisco, CA, USA). After three monthly injections, the CNV was inactive without surrounding exudation and hemorrhage, and the visual acuity was maintained at 20/60 in the left eye (Fig. 1F).
Although retrobulbar injections are generally regarded as safe, routine procedures, a wide variety of complications may occur. The incidence of ocular penetration/perforation during retrobulbar and peribulbar injection has been reported to be between 1/1,000 and 1/4,000 [2]. Risk factors for globe penetration/perforation during retrobulbar or peribulbar anesthesia include axial myopia, the presence of a posterior or inferior staphyloma, multiple injections, a history of a previous scleral buckling procedure, and enophthalmos [3]. The patient in this case had no known risk factors other than a long axial length of 25.34 mm in the left eye.
There are a limited number of reports of CNV development secondary to choroidal ruptures occurring due to open eye injuries. However, there was only one case report of CNV development after ocular penetration/perforation that occurred during retrobulbar anesthesia [2]. In that case, intravitreal ranibizumab was administered as three monthly injections. The CNV had regressed at the 6-month follow-up after the injections. We have presented a rare case of pars plana vitrectomy for scleral penetration/perforation and vitreous hemorrhage that developed during retrobulbar anesthesia, followed by macular CNV occurrence after one year, which was treated using three intravitreal bevacizumab injections. After treatment, the CNV was inactive, but visual acuity did not improve.
To conclude, if globe penetration/perforation during local retrobulbar or peribulbar anesthesia occurs, we should keep in mind that CNV can develop as long as one year afterwards. If CNV develops after globe penetration/perforation during local retrobulbar or peribulbar anesthesia, anti-vascular endothelial growth factor treatment, such as bevacizumab, should be administered to prevent further visual decline. Further studies including a larger number of cases are needed to assess the long-term treatment outcomes and visual prognosis.
 PDF Links
PDF Links PubReader
PubReader ePub Link
ePub Link Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






