


Dry eye syndrome, or dry eye disease, is one of the most common reasons for patient visits to eye clinics. It is a multifactorial disease of the tears and ocular surface, resulting in discomfort, visual disturbances, and tear film instability, and it can potentially damage the ocular surface [1]. A comparison of age-specific prevalence data showed that the prevalence of dry eye syndrome ranged from 5% to more than 35% at various ages [2,3]. People with dry eye are significantly more likely to report problems with reading, performing professional work, computer use, and driving compared to people without dry eye [4].
A major mechanism of dry eye pathogenesis is hyperosmolarity, which is caused by tear deficiency or excessive tear evaporation or both. Hyperosmolarity stress is associated with a potent inflammatory response. Osmotic stress that is initiated by an increase in extracellular osmolarity occurs during normal cellular function in various tissues, including human conjunctival [5,6,7] and corneal epithelial cells [8,9,10]. Tear hyperosmolarity is considered a causative factor in the ocular surface inflammation, cell damage, and irritation symptoms experienced by dry eye syndrome patients [11]. Extracellular hyperosmolarity is also believed to play a role in the inflammatory response [12]. Notably, these symptoms are also strongly associated with inflammatory cytokine secretion. Inflammatory cytokines that are linked to hyperosmotic stress-related pathologies include the tumor necrosis factor (TNF) family and interleukins [12,13].
Diquafosol ophthalmic solution (3%) is a pharmaceutical drug used for the treatment of dry eye syndrome with a novel mechanism of action. It has been widely used in clinical practice to treat dry eye and is currently approved in Japan and South Korea. Diquafosol is a purinergic P2Y2 receptor agonist that promotes tear and mucin secretion in experimental dry eye models [14]. However, little is known about the therapeutic potential of diquafosol on the hyperosmotic stress-induced inflammatory response. The present study is focused on the effects of diquafosol on TNF-α and interleukin-6 (IL-6) expression in hyperosmotic stress-activated human corneal epithelial cells (HCECs).
Materials and Methods
Reagents
Anti-TNF-α and anti-IL-6 antibodies were purchased from Abcam (Cambridge, MA, USA). Anti-β-actin and anti-Lamin B1 antibodies were purchased from Santa Cruz Biotechnology (Santa Cruz, CA, USA). Antibodies against phospho-inhibitor of κB (I-κB) α, I-κBα, phospho-nuclear factor-kappa B (NF-κB) p65, and NF-κB p65 were purchased from Cell Signaling Technology (Beverly, MA, USA). Horseradish peroxidase-conjugated goat anti-rabbit and rabbit anti-goat IgG were purchased from Zymed Laboratories (San Francisco, CA, USA). The annexin V and dead cell assay kit was purchased from Merck Millipore (Billerica, MA, USA). Diquafosol was obtained from Santen (eye drops 3%; Santen Pharmaceutical, Osaka, Japan).
Cell culture and in vitro model of hyperosmotic stress
HCECs (2.040 pRSV-T) were purchased from the American Type Culture Collection (Manassas, VA, USA). Cells were maintained in DMEM/F12 containing 10% Fetal Bovine Serum (Gibco, Carlsbad, CA, USA), 5 µg/mL insulin, 5 µg/mL human transferrin, 5 nM selenium, and 1% penicillin/streptomycin. Cultures were incubated at 37℃ with 5% CO2. Hyperosmotic stress was induced by transferring HCECs from isosmotic (312 mOsm/kg) DMEM/F-12 growth media to hyperosmotic growth media (500 mOsm/kg).
Cell viability and apoptosis assays
To evaluate viability, cells were cultured in a 96-well plate and grown to 80%-90% confluence. HCECs were treated with various concentrations of diquafosol solution for 20 hours. After incubation, cell viability was determined by using the CCK-8 assay (Dojindo Laboratories, Kumamoto, Japan). Color development was measured at 450 nm using an ELISA microplate reader (Infinite M200; Tecan, Männedorf, Switzerland). Experiments were performed in triplicate. The percentage of apoptotic cells was determined with the annexin V and dead cell kit, according to the manufacturer's instructions. Briefly, harvested cells were washed with PBS and then mixed with 100 µL of the annexin V and dead cell assay kit reagents. Samples were incubated at room temperature for 20 minutes in the dark. Measurements were conducted in triplicate using a MUSE cell analyzer (Merck Millipore, Billerica, MA, USA).
RNA isolation and quantitative real-time polymerase chain reaction
To determine the a mount of mRNA expression, cells were exposed to hyperosmotic media (500 mOsm/kg DMEM/F-12, serum-free) for 30 minutes, followed by diquafosol for 4 hours, as previously described [15]. Total RNA was isolated from the cells with Trizol reagent (Life Technologies, Rockville, MD, USA), according to the manufacturer's instructions, and reverse-transcribed into complementary DNA with M-MLV reverse transcriptase (Promega, Madison, WI, USA). Real-time polymerase chain reaction (PCR) was performed using SYBR Premix Ex Taq (Perfect Real Time) Premix (Takara Bio, Otsu, Japan) and Takara Thermal Cycler Dice (TP850), according to the manufacturer's protocol (Takara Bio, Shiga, Japan). Relative quantification of mRNA expression was performed using TP850 software. Table 1 shows the gene-specific primers used in this study (Macrogen, Seoul, Korea). PCR products were electrophoresed on 1% agarose gels and visualized by GreenLight (BioAssay Co., Daejeon, Korea). PCR conditions are indicated in Table 1. All experiments were performed in triplicate.
Western blot analysis
To determine the expression of proteins, cells were exposed to hyperosmotic media (500 mOsm/kg DMEM/F-12, serum-free) for 30 minutes, followed by diquafosol for 24 hours. Protein extraction and western blotting were performed as described previously [15]. Membranes were incubated overnight at 4℃ with polyclonal antibodies against TNF-α and IL-6 and with a monoclonal antibody against β-actin in 0.1% Tween-20 Tris-buffered saline (TBS) containing 5% nonfat dried milk.
Membranes were then incubated with the appropriate horseradish peroxidase-conjugated secondary antibodies for 1 hour. Antibody binding was visualized using an enhanced chemiluminescence detection kit (ELPIS Biotech, Daejeon, Korea) and exposure to X-ray film. The experiments were performed in triplicate. Quantification of band intensity was performed using ImageJ software ver. 1.52 (National Institutes of Health, Bethesda, MD, USA).
Cytoplasmic and nuclear protein extraction
To confirm the activation of NF-κB, cells were exposed to hyperosmotic media (500 mOsm/kg DMEM/F-12, serum- free) for 30 minutes, followed by diquafosol for 30 minutes. Proteins from the cytoplasm and nucleus were separated by using the NE-PER nuclear and cytoplasmic extraction reagent kit (#78835; ThermoFisher Scientific, Waltham, MA, USA). Brief ly, HCECs were harvested, cells were centrifuged at 16,000 × g for 5 minutes, and the supernatant was removed. Ice-cold CER-I and -II solutions were added to the pellet per the manufacturer's instructions to separate cytoplasmic proteins from nuclear-compartment proteins. Western blots for NF-κB, p-NF-κB, I-κB, p-I-κB, β-actin (as a cytosol marker) and Lamin B1 (as a nuclear marker) were performed to ensure that there was no contamination.
Immunofluorescence staining
Harvested cells were fixed with 10% neutral buffered formalin solution at room temperature for 10 minutes. Cells were per meabilized wit h 0.3% Tr iton X-100 for 15 minutes and blocked overnight with 5% normal goat serum and bovine serum albumin in TBS at 4℃. Cells were then incubated with primary antibodies specific for TNF-α, IL-6, and p-NF-κB (diluted 1 : 50 to 1 : 100) in 5% bovine serum albumin overnight at 4℃ and washed three times in TBS. Cells were then incubated with the appropriate Alexa Fluor 488- or 555-conjugated secondary antibody at room temperature for 1 hour in the dark; nuclei were then counterstained with 4′,6-diamidino-2-phenylindole (DAPI, 1 µg/mL). Slides were mounted with ProLong Gold (ThermoFisher Scientific, Waltham, MA, USA), and images were captured by fluorescence microscopy (Axio Vision 4; Carl Zeiss, Jena, Germany). Fluorescence intensity was measured using color histograms generated with ImageJ software.
Statistical analysis
Data were evaluated by one-way analysis of variance using Tukey's post-hoc test. Analyses were performed using GraphPad PRISM software ver. 5.02 (GraphPad PRISM Software Inc., La Jolla, CA, USA). The criterion for statistical significance was set at p < 0.05. All statistical tests were two-tailed.
Results
Effects of diquafosol ophthalmic solution on the viability of HCECs
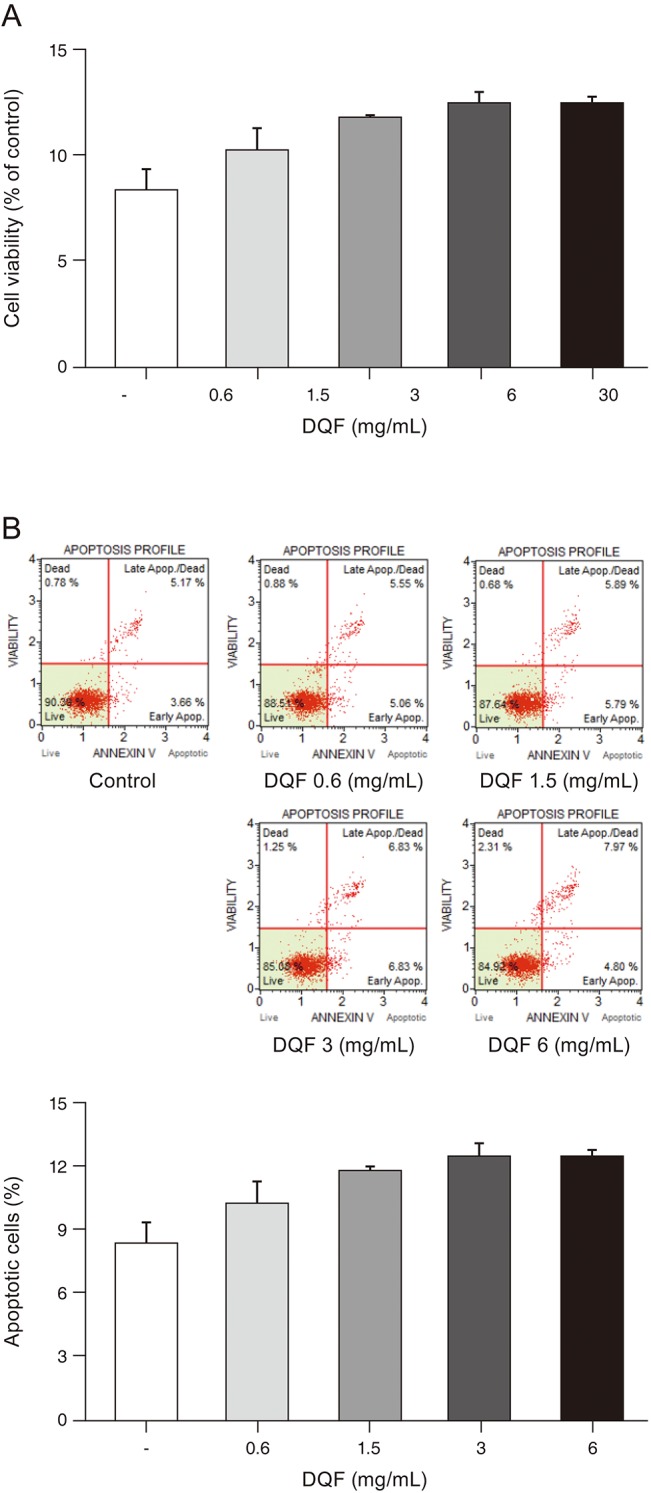
To investigate the cytotoxicity of diquafosol ophthalmic solution, we measured cell viability using the CCK-8 assay kit. Diquafosol displayed a dose-dependent toxicity in HCECs under starved conditions. No significant toxicity was observed at diquafosol concentrations of up to 6 mg/mL. However, cell viability notably decreased when HCECs were exposed to 30 mg/mL of diquafosol (Fig. 1A). We also measured the effects of diquafosol on apoptosis. Relative to control cells, the percentage of apoptotic HCECs increased with diquafosol in a dose-dependent manner, but the change was small and not significant (Fig. 1B).
Effects of diquafosol on hyperosmotic stress-induced TNF-α and IL-6 expression
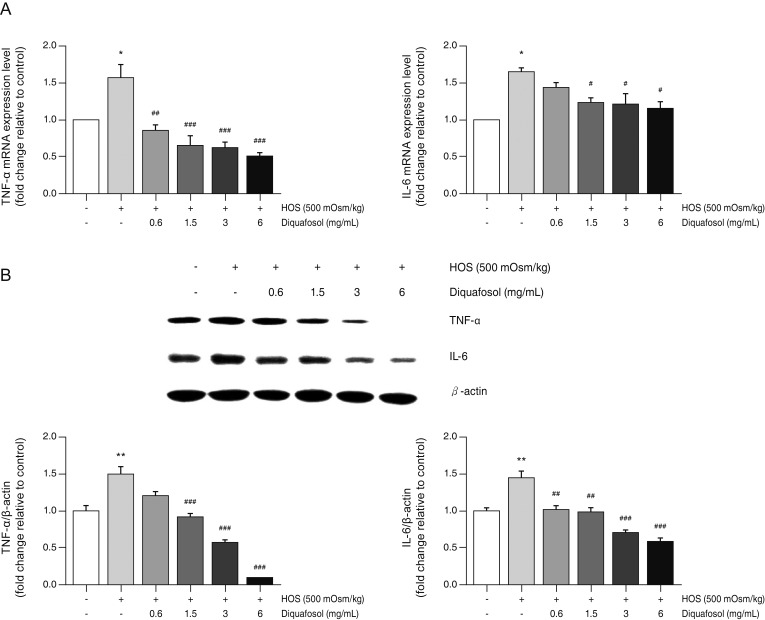
To evaluate the anti-inflammatory activity of diquafosol, we investigated the effects of diquafosol on hyperosmotic stress-induced inflammatory gene expression. Real-time PCR analysis showed an increase in hyperosmotic stress-induced TNF-α and IL-6 mRNA concentration (Fig. 2A). However, pretreatment with diquafosol (1.5-6 mg/mL) resulted in the attenuation of the inflammatory response. In addition, western blot results revealed that TNF-α and IL-6 protein levels were markedly decreased by diquafosol in hyperosmotic stress-induced inflammation (Fig. 2B).
Suppression of hyperosmotic stress-induced TNF-α and IL-6 expression by diquafosol
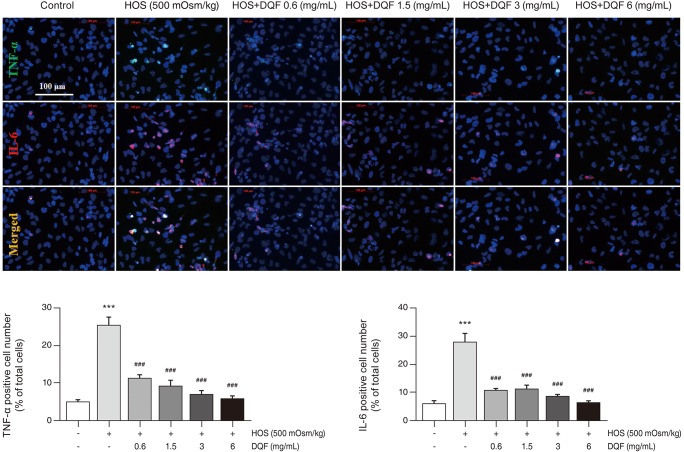
Non-hyperosmotic stress-stimulated cells exhibited weak staining, suggesting low basal levels of TNF-α and IL-6 (Fig. 3). After hyperosmotic stress stimulation, immunocytochemistry analysis revealed that TNF-α and IL-6 expression increased significantly. Diquafosol appears to block expression of TNF-α and IL-6 proteins in HCECs in response to hyperosmotic stress.
Effects of diquafosol on the NF-κB signaling pathway in hyperosmotic stress
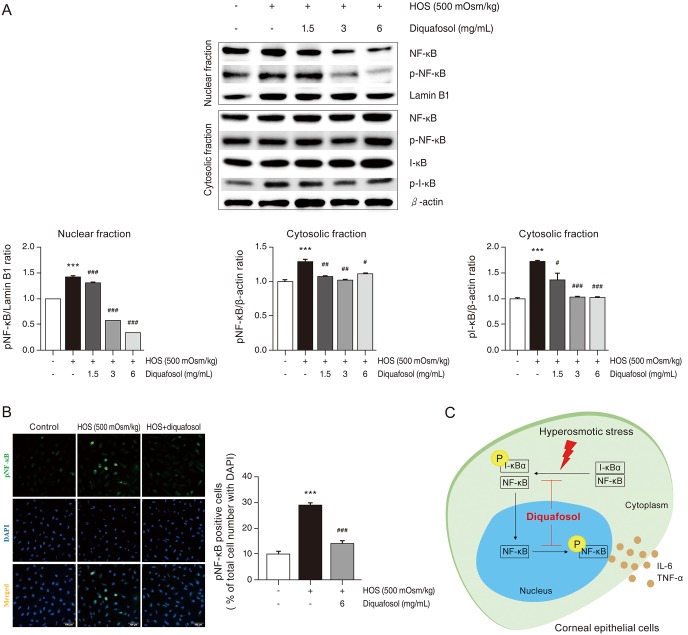
The NF-κB signaling pathway contributes to the inflammatory process of dry eye, so we investigated the effects of diquafosol on hyperosmotic stress-induced NF-κB activation. Phosphorylation of I-κB and nuclear translocation of NF-κB p65 were notably increased by hyperosmotic stress, whereas treatment with diquafosol decreased the hyperosmotic stress-induced levels of p-I-κB and nuclear translocation of NF-κB p65 in a dose-dependent manner (Fig. 4A). Hyperosmotic stress resulted in the translocation of p-NF-κB-p65 to the nucleus as seen by immunocytochemistry. Incubation with anti-NF-κB-p65 showed marked nuclear staining in HCECs under hyperosmotic stress conditions, whereas cells treated with diquafosol (6 mg/mL) showed only background staining (Fig. 4B). The action of diquafosol through inhibiton of NF-κB activity is schematically summarized (Fig. 4C).
Discussion
Dry eye disease is the most common disorder of the eye, and its associated symptoms can cause corneal injury [16]. Dry eye disease is a condition caused by deficient tear production or an excessive loss of water from the tear film by evaporation. Increased tear osmolarity has been recognized as a hallmark of dry eye syndrome, and it appears to play an important role in the pathogenesis of ocular surface damage. Tear osmolarity has been reported to be the single best marker for dry eye disease [17,18]. Tear film hyperosmolarity may cause pathological changes in the corneal epithelium, such as desquamation, fewer intercellular connections, loss of microplicae, cell membrane disruptions, and cellular swelling with decreased cytoplasmic density [19]. Other studies have reported that hyperosmotic stress not only stimulates the expression and production of inflammatory cytokines TNF-α, IL-8, and IL-1 in HCECs in vitro [8,9], but also stimulates the expression of these inflammatory mediators in an experimental dry eye mouse model in vivo [20]. Other studies have also shown that hyperosmolarity induces the expression of inflammatory cytokines such as TNF-α, IL-6, and monocyte chemotactic protein-1 (MCP-1) in cultured HCECs [10,21]. In addition, an increase in these proteins has been seen in an HCEC culture model, an in vivo murine dry eye model, and in the tears of dry eye patients [22,23].
The protective properties of diquafosol have been recognized in the treatment of dry eyes. Diquafosol stimulates the production of water, lipids, and mucin by activating the purinergic (P2Y2) receptor on the ocular surface [24]. However, little is known about the bioactivity and potential clinical implications of diquafosol on hyperosmotic stress-induced inflammation. In this study, we present evidence that diquafosol may exert beneficial effects on dry eye-mediated ocular inflammation. We show that diquafosol significantly suppressed the expression of inflammatory cytokines TNF-α and IL-6 in HCECs exposed to hyperosmotic stress. Our f indings demonstrate that hyperosmotic stress induces inflammation, and diquafosol is an effective agent that protects HCECs from hyperosmotic stress-induced inflammation. These results are consistent with previous studies in which the secretion of inf lammatory cytokines was signif icantly reduced in desiccation stress-induced dry eye models [25]. Results showing that diquafosol inhibits the production of inflammatory cytokines in a variety of dry eye models suggest that diquafosol may exert anti-inflammatory effects on various pathogenic factors associated with dry eye syndrome, such as tear hyperosmolarity or dry conditions.
NF-κB is a key transcription factor in the inflammatory response of various cells, and it could play an important role in the production of cytokines that have been implicated in the pathogenesis of dry eye disease. NF-κB dimers are retained in an inactive form in the cytosol, bound by I-κB proteins. Under various stimuli, including hyperosmotic stress, phosphorylation, and subsequent degradation of I-κB proteins occurs, allowing NF-κB to translocate to the nucleus where it activates various inflammatory genes [26]. In addition, phosphorylation of NF-κB subunits affects NF-κB transcriptional responses. Phosphorylation of t he p65 subunit of NF-κB leads to t he selective t ranscription of downstream inf lammatory cytokines [27]. Desiccating stress causes NF-κB activation in an in vivo model of dry eye disease; conversely, NF-κB inhibitors reduce IL-1β and IL-6 production and corneal epithelial damage in mice [28]. Through in vitro experiments using HCEC cells, we confirmed that NF-κB phosphorylation and nuclear localization are responses to hyperosmotic stress. Our results suggest that the activated NF-κB signaling pathways in our experimental dry eye model may play a role in the induction of inflammatory cytokines IL-6 and TNF-α. Previous studies reported that NF-κB inhibitors are useful for treating dry eye disorders and other disorders requiring the wetting of the eye. In our study, hyperosmotic stress-induced expression of p-NF-κB and p-I-κB and degradation of I-κB were blocked by diquafosol, which agrees with the results of immunocytochemistry analyses that show a significant nuclear translocation of p-NF-κB.
Our findings suggest potential benefits of diquafosol treatment in ocular surface disorders such as dry eye. Diquafosol partially protects the human corneal epithelium from hyperosmotic stress-induced inflammatory responses by reducing TNF-α and IL-6 levels. Diquafosol is a purinergic P2Y2 receptor agonist and enhances the corneal barrier function by increasing tear fluid secretion in dry eye disease [29]. However, inflammatory cytokines also contribute to dry eye disease [30]. Therefore, the inhibition of IL-6 and TNF-α protein expression indicates that diquafosol treatment may also improve dry eye symptoms, at least partly, through anti-inflammatory mechanisms. NF-κB inhibitors have been reported to inhibit pro-inflammatory cytokine production as well as reverse corneal epithelial damage [28]. A correlation between NF-κB inhibition and corneal epithelial recovery suggests that the anti-inflammatory effects of diquafosol can act as a partial mechanism to improve dry eye symptoms.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






