

Retinal detachment associated with macular hole mostly occurs in highly myopic eyes [1,2]. Although the mechanisms are not fully understood, it has been suggested that macular hole retinal detachment (MHRD) is caused by tangential and anteroposterior traction due to presence of a posterior staphyloma combined with weakened retinal adhesion caused by retinal pigment epithelium atrophy [2,3]. These background pathologies make MHRD complicated in high myopia a surgical challenge.
Various surgical procedures including macular buckling [4,5], pars plana vitrectomy (PPV) with tamponade using gas or silicone oil [6,7], and extramacular drainage [8] have been reported to improve MHRD surgery outcomes. PPV with internal limiting membrane (ILM) peeling and gas tamponade has been one of the most popular surgical procedures for MHRD because it effectively relieves tangential macular traction by removing all the overlying fibrous membrane adjoining the macular hole (MH) [9,10,11]. Recently, various ILM manipulations that covered the MH were reported to increase the primary success rate of MHRD surgery up to 100% [12,13,14]. These diverse adjunctive procedures appeared to improve reattachment and MH closure rates as well as functional outcomes. However, these studies examined surgical outcomes over a relatively short period of time and did not report long-term results. In addition, the impact of MH closure on functional outcomes during long-term follow-up was not investigated.
As highly myopic eyes are prone to degenerative changes causing visual loss, the functional outcomes of MHRD surgery should be evaluated over a long period. The purpose of this study was to investigate long-term visual acuity changes after surgical reattachment of MHRD in highly myopic eyes.
Materials and Methods
The medical records of patients who underwent PPV for MHRD between November 2008 and October 2015 at Pusan National University Hospital were retrospectively reviewed. The study design was approved by the institutional review board of Pusan National University Hospital (1812-020-074), and the study was conducted following the principles outlined in the Declaration of Helsinki. The informed consent was waived due to the retrospective nature of the study.
Patient inclusion criteria were as follows: (1) clinical presentation of MHRD in a highly myopic eye, (2) MH as the primary cause of retinal detachment, (3) 3-port PPV treatment, and (4) reattachment maintained for Ōēź3 years after surgery. Eyes in which MH was not considered the primary cause of retinal detachment were excluded based on configuration of subretinal fluid and presence of breaks other than MH. High myopia was defined as refractive error ŌēźŌłÆ6.0 diopters without refractive surgery or axial length Ōēź26.5 mm.
The cohort of 106 eyes was obtained by database search for ŌĆśmacular holeŌĆÖ and ŌĆśretinal detachmentŌĆÖ between November 2008 and October 2015 regardless of refractive error or axial length. Among them, 64 eyes were highly myopic and underwent PPV for MHRD. Twenty-three eyes were followed up over 3 years, and one eye was excluded due to reattachment failure. Finally, 22 eyes were included in the following analysis. Of the 22 total eyes, 20, 19, and 18 eyes were followed up at postoperative 6 months, 1 year, and 2 years, respectively. The clinical data collected from each case record were patient age; sex; preoperative best-corrected visual acuity (BCVA); postoperative BCVA at 6 months and 1, 2, and 3 years; axial length; posterior staphyloma presence; lens status; and operative variables including use of conventional ILM peeling or the inverted ILM flap technique, tamponade types, MH closure, and retinal reattachment.
All operations were conducted by experienced vitreoretinal surgeons (JEL and SWP). Conventional 20-, 23-, or 25-gauge 3-port PPV (Constellation, Alcon, Fort Worth, TX, USA) was performed. Posterior vitreous detachment was created by vitreous aspiration using a cutter or extrusion needle. After removing the vitreous to the periphery as much as possible, the viscous submacular fluid was gently drained through the MH or extramacular sites. If there was no preexisting peripheral break, then retinotomy was performed outside of the macula to avoid chorioretinal atrophy, and one low-barrier photocoagulation was performed around the retinotomy site.
The ILM was stained with indocyanine green or brilliant blue G for ILM removal or flap technique. For the ILM flap technique, a portion of the ILM about 1-disc diameter in size was left at the superior margin of the MH and inverted as a single layer. The inverted flap was stabilized with perfluoro-n-octane (Perfluoron, Alcon) during fluid-air exchange. The vitreous was replaced by long-acting gas (sulfur hexaf luoride [SF6] or perf luoropropane [C3F8]) at a non-expanding concentration or silicone oil at the surgeon's discretion. Patients were advised to stay in a strict face-down position for 1 to 7 days after surgery.
To confirm reattachment and MH closure, optical coherence tomography (OCT) examinations were performed in all patients before and after surgery using spectral-domain (Cirrus HD-OCT, Carl-Zeiss, Dublin, CA, USA) or swept-source (DRI-OCT Atlantis, Topcon, Tokyo, Japan) OCT devices. MH closure was defined as absence of a neurosensory defect at the fovea. Primary attachment was defined as retinal reattachment without requiring additional surgical procedures except silicone oil removal. Patients were divided into two groups based on MH closure.
Visual acuity by a Snellen chart was converted to logarithm of the minimum angle of resolution (logMAR) for analysis. Values are reported as the mean and standard deviation. Wilcoxon signed-rank test was conducted to evaluate postoperative changes for each group. Mann-Whitney U-test and Fisher's exact test were used to compare continuous and categorical variables between two groups, respectively. A p-value <0.05 was considered significant. All analyses were performed using IBM SPSS Statistics ver. 21.0 (IBM Corp., Armonk, NY, USA).
Results
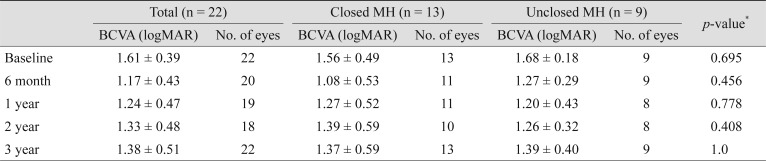
This study included 22 eyes of 22 patients with MHRD who underwent PPV. Patient characteristics are shown in Table 1. Patients comprised one male and 21 females with a mean age of 61.8 ┬▒ 10.1 years. At baseline, mean BCVA was 1.61 ┬▒ 0.39 logMAR, and mean axial length was 28.96 ┬▒ 1.57 mm. All patients had staphyloma. Concurrent phacoemulsification was performed in 12/14 (85%) phakic eyes. After primary surgery, two eyes remained phakic. One of the phakic eyes had no significant cataract progression during follow-up, whereas phacoemulsification was performed in the other eye at one year after initial MHRD surgery. PPV with conventional ILM peeling was conducted in 19 eyes, and PPV with the inverted ILM flap technique was performed in three eyes. The vitreous was replaced with C3F8 in 14 (63.6%) eyes, SF6 in three (13.6%) eyes, and silicone oil in five (22.7%) eyes.
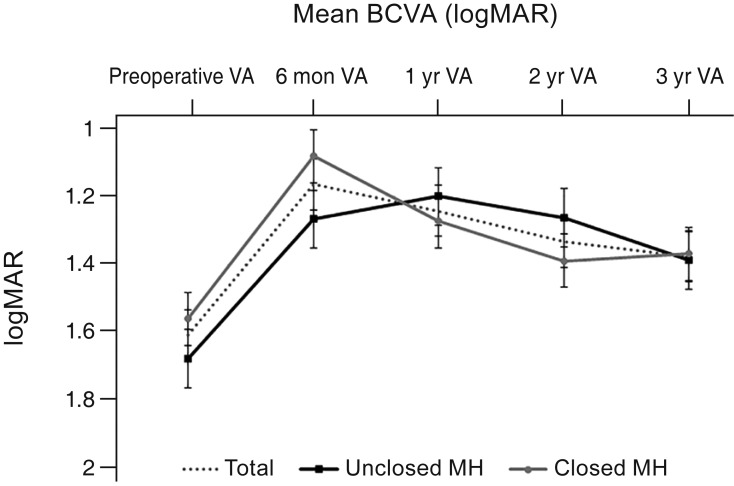
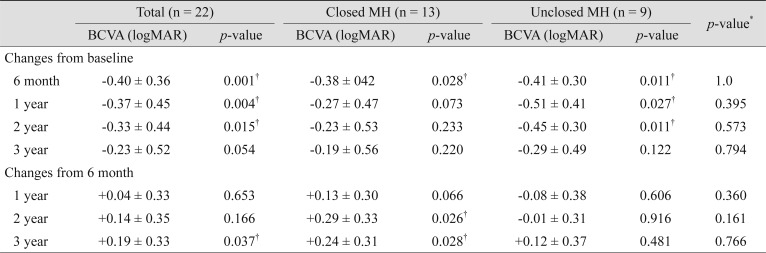
The retina was reattached in all eyes (n = 22) with a single surgery, excluding the silicone oil removal operation. The MH was closed in 13 eyes (59.1%) and unclosed in nine eyes (40.9%). The mean BCVA significantly improved from 1.61 ┬▒ 0.39 logMAR preoperatively to 1.17 ┬▒ 0.43 logMAR at 6 months postoperatively (p = 0.001). At 3 years postoperatively, patient visual acuity gradually decreased to 1.38 ┬▒ 0.51 logMAR, and the improvement was no longer significant (p = 0.054) (Table 2). Compared with visual acuity at 6 months, that at 3 years significantly decreased (p = 0.037) (Fig. 1).
Comparison of closed and unclosed MH groups
Comparisons of the preoperative clinical characteristics between the closed and unclosed MH groups are shown in Table 1. There were no significant differences between the two groups with respect to patient sex, age, preoperative BCVA, axial length, posterior staphyloma presence, lens status, or operative technique.
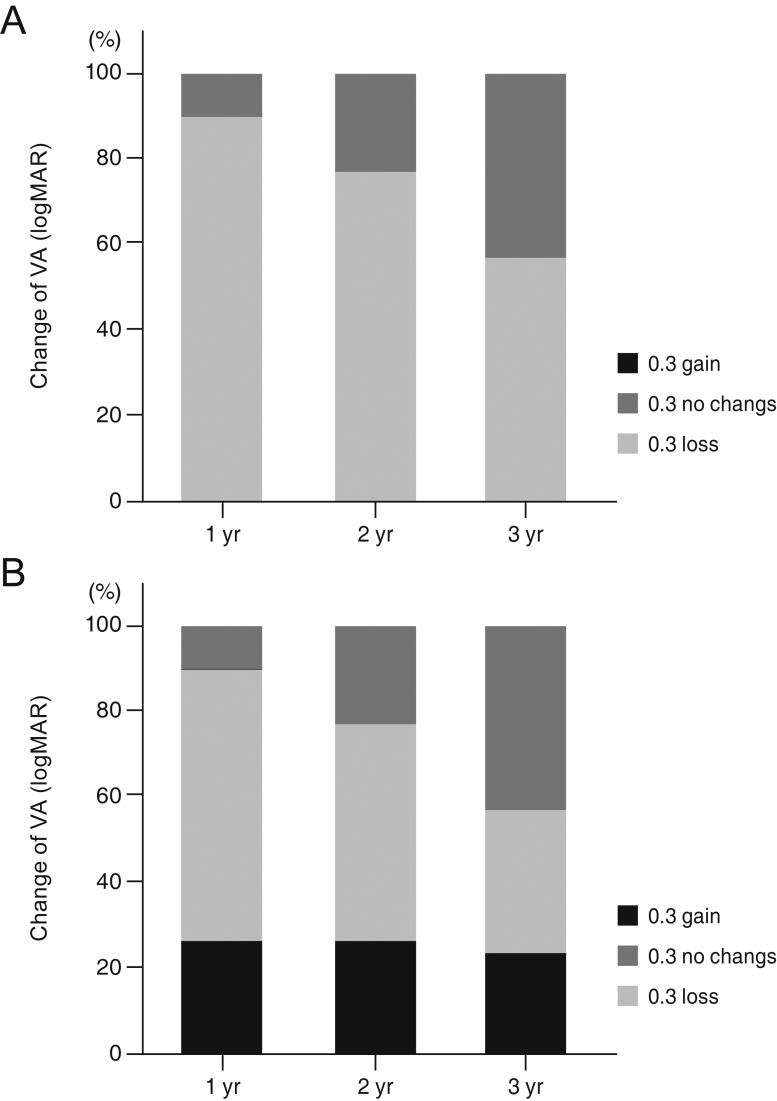
There was a significant improvement of the visual acuity of the closed and unclosed MH groups at 6 months after surgery (p = 0.028 and 0.011, respectively). The mean loss of visual acuity at 3 years compared with that at 6 months after surgery was 0.24 ┬▒ 0.31 and 0.12 ┬▒ 0.37 logMAR in the closed and unclosed MH groups, respectively (Table 3). There was no significant difference in mean visual acuity loss between the two groups (p = 0.766). The number of eyes that had decreased visual acuity by Ōēź0.3 logMAR at 3 years compared with 6 months after surgery was five in the closed (38%) and four in the unclosed (44%) MH groups (p = 1.0) (Table 4 and Fig. 1, 2A, 2B).
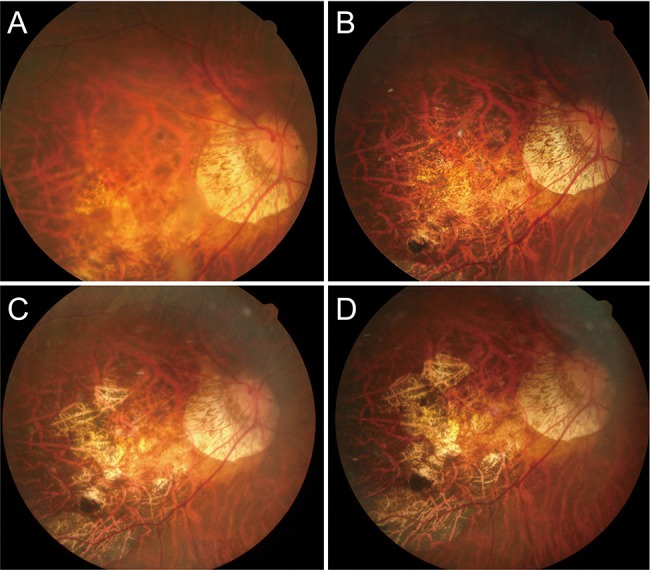
In one eye with an unclosed MH after primary surgery, a secondary surgery was performed to close the MH. The primary surgery was PPV combined with phacoemulsification, the ILM peeling technique, and C3F8 tamponade. Although the retina was reattached, the MH remained open. An additional surgery was performed 3 months after the primary surgery, and the ILM was further removed and the vitreous cavity was filled with SF6. However, the MH remained open after the second operation. Visual acuity was maintained for 2 years after primary surgery. However, at 3 years, it decreased because of expanding chorioretinal atrophy (Fig. 3A-3D).
Analysis of the long-term vision loss subgroup
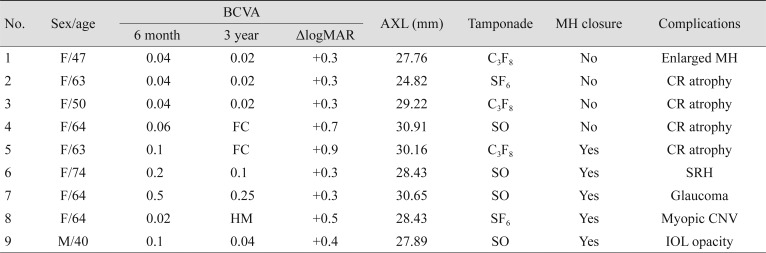
Table 4 provides a summary of nine patients with BCVA loss Ōēź0.3 logMAR at 3 years compared with 6 months after surgery. The most common cause of BCVA loss was enlargement or development of chorioretinal atrophy. There were two cases of subretinal hemorrhage that were related to myopic choroidal neovascularization (CNV) and lacquer crack formation, respectively. One eye had vision loss from open-angle glaucoma, which developed following vitrectomy with silicone oil tamponade. Only one eye had significant vision loss that was suspected to be caused by a persistent MH, with elevated edges and macular edema. In this eye, the horizontal diameter of the MH increased from 1,050 ┬Ąm at 6 months to 1,249 ┬Ąm at 3 years, whereas its height decreased from 481 to 428 ┬Ąm, accompanied by a decrease in Snellen acuity from 0.04 to 0.02. Another one eye showed vision loss from intraocular lens calcification, and vision was recovered to the same level as at postoperative 6 months after intraocular lens exchange surgery. Statistical analysis using the improved vision of the case showed no difference between the two groups at 3 years, and vision loss compared to that at 6 months remained significant.
Discussion
PPV with gas tamponade has been considered the primary surgical treatment for MHRD since the report by Gonvers and Machemer [15]. Although retinal reattachment had a fair success rate using this method, the hole closure rate remained unsatisfactory because of degenerative pathology associated with high myopia [16,17]. After introduction of various ILM manipulations, such as ILM peeling and the ILM flap technique, the primary success rate has increased, resulting in better visual outcomes [10,12,13,14]. However, because degenerative pathology persists in highly myopic eyes after MHRD surgery, patients are prone to vision loss caused by complications including chorioretinal atrophy, lacquer crack hemorrhage, and myopic CNV. The present study aimed to investigate long-term MHRD surgery outcomes and found that postoperative visual improvement was not maintained at 3 years regardless of MH closure.
MH closure is thought to be a key factor for anatomical success by restoring the normal anatomical configuration of the macula and reducing the chances of MH-related retinal detachment recurrence [3]. Accordingly, many investigators presumed that MH closure would also promote better visual acuity in MHRD (e.g., idiopathic MHs). However, the better functional outcomes observed in interventional groups would be biased by a higher reattachment rate. Moreover, the association between MH closure and visual acuity improvement after MHRD surgery was inconsistent between previous reports. Nakanishi et al. [18] reported that there were no significant differences in postoperative BCVA between closed or unclosed MHs after PPV and ILM peeling with gas tamponade. Nishimura et al. [7] and Nadal et al. [19] also reported no significant differences in postoperative BCVA between eyes with and without MH closure after PPV with silicone oil tamponade. However, Ikuno et al. [20] and Lam et al. [21] reported that postoperative BCVA was significantly better in patients with MH closure than in those without MH closure after PPV with or without ILM peeling combined with C3F8.
In the present study, MH closure was unrelated to longterm visual outcomes after MHRD surgery in highly myopic eyes, and recurrence of retinal detachment was not observed even in unclosed MH groups. The pattern of visual acuity changes was similar between the two groups. Visual acuity peaked at 6 months to 1 year after surgery and then gradually decreased until visual improvement was no longer significant at 3 years. Nine patients had BCVA loss Ōēź0.3 logMAR at 3 years compared with 6 months after surgery. Postoperative visual improvement in our study was related to macular attachment, as significant improvement was observed in both groups. By contrast, vision loss was related to various complications including enlargement of chorioretinal atrophy, macula thinning, subretinal hemorrhage, open-angle glaucoma, and myopic CNV. Most of these complications are associated with the nature of degenerative myopia. Nevertheless, close follow-up after surgery is important for timely intervention as myopic CNV may reduce the vision loss [22].
Maintaining retinal reattachment is important in terms of visual function, but it remains unclear whether additional surgery for closing flat-open MH is necessary when the retina is reattached. The results of this study failed to provide enough evidence to recommend additional surgery. Even when the MH remained open, retinal detachment seemed to rarely recur during long-term follow-up after the acute phase. MH closure does not appear to have a significant effect on long-term visual acuity. However, there was one case of vision loss related to MH enlargement. Moreover, three of four cases with vision loss in the open MH group were related to chorioretinal atrophy. Considering that our observations were limited to 3 years, a longer follow-up period might have resulted in a significant difference between the two groups. Consequently, the decision to incorporate additional surgery should be based on various factors including presence of useful vision, history of recurrence, risk of further macular damage, and tissue availability for flap techniques [23,24].
This study had several limitations. The study was retrospective, and the number of included eyes was relatively small. The observation period was 3 years, which may not be sufficient to assess long-term MHRD surgery results as degenerative myopia is a life-long condition. Further studies incorporating a larger number of eyes and longer follow-up periods are needed to verify the results.
In conclusion, this study showed that visual acuity tended to decrease from 6 months to 3 years after surgery. Vision loss was associated with the nature of degenerative myopia, and favorable effects of MH closure were not observed on visual outcomes during the long-term follow-up period of 3 years. Additional surgery for MH closure in patients with high myopia is controversial when the retina is reattached and the MH remains open.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






