A Case of Rothia mucilaginosa Keratitis in South Korea
Article information
Dear Editor,
Bacterial keratitis is the most common cause of suppurative corneal ulceration, which can lead to visual impairment and frequently presents as an ocular emergency. Rothia mucilaginosa (R. mucilaginosa), previously known as Stomatococcus mucilaginosus, is a Gram-positive, coagulase-negative coccus of the family Micrococcaceae [1]. R. mucilaginosa is known as normal flora of the upper respiratory tract and oral cavity. It has been reported to be the causative agents of several diseases such as bacteremia, endocarditis, and urinary tract infection [1]. Recently, it is increasingly recognized as a pathogen associated with ocular infection. To our knowledge, only one keratitis case was reported with Kocuria palustris and R. mucilaginosa in vitamin A deficiency. We report a case of bacterial keratitis caused only by R. mucilaginosa, identified by 16S rRNA gene sequence analysis.
An 89-year-old man presented to Chonbuk National University Hospital with pain in his left eye after walking in mountains to pick up chestnuts 25 days ago. He had diabetes mellitus and underwent cataract surgery in both eyes 8 years before. At initial visit, visual acuity was light perception in his left eye. Slitlamp examination showed severe ciliary injection, a 5.0 × 4.5 mm sized central corneal epithelial defect with deep stromal infiltration, and moderate anterior chamber reaction with hypopyon (Fig. 1A, 1B). A B-scan ultrasound of the fundus of the left eye was unremarkable. Under diagnosis of corneal ulcer, corneal scraping for culture was done immediately. He was admitted and started on topical vancomycin 2.5% and ceftazidime 5% eye drops every hour as well as ofloxacin 0.3% ointment. He received intravenous flomoxef (1 g/day) simultaneously. On the 3rd day of hospitalization, corneal epithelial healing began, but anterior chamber reaction and stromal infiltration persisted. On the 8th day, as ocular inflammation gradually decreased, medical treatment was tapered. He was discharged 10 days after initial treatment with a remaining small epithelial defect and mild anterior chamber reaction. The culture of the ulcer grew catalase-positive, Gram-positive cocci forming white colonies. Finally, R. mucilaginosa was identified by 16s rRNA sequencing analysis. The criterion for gene sequence identif ication is homology >98% (ABI plasma 3730XL; Genotek, Kanata, ON, Canada). Two months after initial treatment, the corneal infiltrate and hypopyon were all resolved (Fig. 1C, 1D). Uncorrected visual acuity improved to 20 / 200.
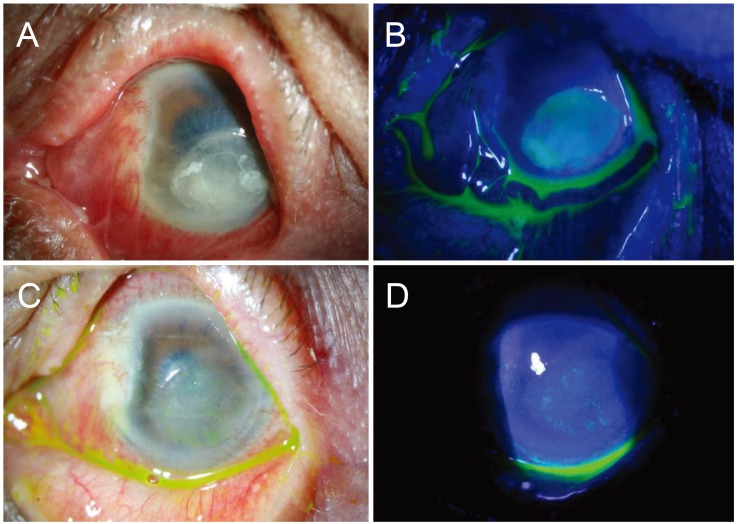
Slit-lamp photographs of Rothia mucilaginosa keratitis at initial presentation. Anterior segment photograph shows severe ciliary injection and chemosis, about a 5.0 × 4.5 mm sized central corneal epithelial defect and stromal infiltration, Descemet's membrane folding, and hypopyon (A,B). Slit-lamp photographs 2 months after initial treatment. Anterior segment photographs show healed epithelial defect, fainted corneal opacity, and peripheral neovascularization (C,D).
R. mucilaginosa is a rarely detected bacterial species in ocular infection. Only four cases have been reported as follows: postoperative endophthalmitis in a 91-year-old man [2], keratitis in a 58-year-old woman with vitamin A deficiency [3], acute postoperative endophthalmitis after phacoemulsification in a 65-year-old woman [4], and late-onset bleb associated endophthalmitis in a 41-year-old man [5]. Evisceration was performed in two postoperative endophthalmitis cases. However, general outcomes due to ocular infection by R. mucilaginosa are unknown due to insufficient clinical reports. Although our case showed relatively good prognosis, unexpected infections can be a harbinger of serious corneal melting. Case reports since 1978 have implicated R. mucilaginosa in several systemic infections among patients who are usually immunocompromised [4]. In a previous R. mucilaginosa keratitis case, the patient suffered severe dry eye owing to an underlying vitamin A deficiency [5]. In our case, the patient was not immunocompromised and had no infectious disease history, other than old age. Although the precise cause remains unknown, one of the possible causes of keratitis is trauma to the cornea due to rubbing. We suspect the patient's hand had been contaminated with saliva suitable for transfer of R. mucilaginosa to the cornea.
R. mucilaginosa is a facultative anaerobic bacterium, but it can also grow under aerobic conditions [4]. However, it is not easy to identify R. mucilaginosa because this rarely isolated species has been often misidentified as streptococcus or coagulase-negative staphylococci [4]. In our case, it was misidentified as coagulase-negative staphylococci at first. We used two automated microbial identification devices called VITEK MS and VITEK2 (BioMérieux, Lyon, France). As the results from both were different, gene sequencing analysis was performed.
To our knowledge, this is the first case of corneal ulcer from R. mucilaginosa in South Korea. If there is difficulty treating an intractable corneal ulcer despite using empirical antibiotics therapy, R. mucilaginosa has to be considered and molecular analysis is an accurate method to identify it.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article were reported.