

Cystoid macular edema (CME) is the most common cause of reduced vision and poor visual outcomes following uncomplicated cataract surgery [1,2,3,4]. While previous reports have shown several identifiable causes [5,6,7,8,9,10,11,12,13], there has been no consensus on the exact etiology of CME in the vast majority of cases [6,14]. We propose that abnormal immediate postoperative intraocular pressure (IOP), an easily preventable etiology not commonly considered, may be a major cause of CME in routine cataract surgery cases.
Materials and Methods
A random block of patients undergoing routine microincision cataract surgery (MICS) by a single surgeon (JJ, Evergreen Eye Center) during a 3-month period from July to September 2008. Three other surgeons participated in IOP testing, but their patients were not examined with ocular coherence tomography (OCT) and thus served as a control group. Verbal informed consent was obtained, and patients chose to have their IOP tested and adjusted in the operating theater. If CME was noted, OCT (Stratus OCT; Zeiss, Dublin, CA, USA) of the macula was tested at 2 weeks and at 6 weeks following the cataract procedure, at no charge to the patient. Institutional review board approval was obtained through the clinical committee at Evergreen Eye Surgery Center, Federal Way, WA. Adjustment of IOP by sterile technique was performed at the conclusion of the MICS cataract procedure using a sterile tip TonoPen (AO Reichert, Buffalo, NY, USA), with a new sterile sleeve used for each patient. If the IOP was considered to be too high (>30 mmHg) or too low (<9 mmHg) or if any wound leaks were present, the IOP was adjusted using a sterile irrigating cannula with balanced salt solution (Allergan, Irvine, CA, USA). If the IOP was between 9 mmHg and 30 mmHg, the pressure was not adjusted but was measured again the following day. Routine preoperative eye drops consisting of cyclopentolate 1% (Cyclogyl; Alcon Laboratories, Fort Worth, TX, USA), ketorolac tromethamine 0.5% (Acular, Allergan), gatifloxicin 1% (Zymar, Allergan), and Neosynephrine 0.5% were instilled per usual preoperative protocol. Postoperative drops including gatifloxicin 1% (Zymar, Allergan), brimonidine 0.1% (Alphagan P, Allergan), and neomycin/polymyxin/dexamethaaone (Maxitrol, Alcon) ointment were instilled so long as no patient allergies were reported. Gentamycin sulfate 20 mg (Henry Schein, Chicago, IL, USA) and methylprednisolone 20 mg (Depo-Medrol, Henry Schein) in 0.5 cc solution was injected in the inferior subconjunctival fornix prior to pressure patching the eye overnight (in over 20,000 cases since this routine was first implemented, the authors observed no cases of endophthalmitisŌĆöhowever we have all now changed to intracameral moxifloxicin [Vigamox, Alcon] antibiotics and no longer give injectibles). The following day, vision testing including a Snellen chart, IOP testing with a TonoPen (AO Reichert, Depew, NY, USA), and slit lamp biomicroscopy was performed in the clinic following removal of the eye patch. An additional 2-week exam was performed on every patient who agreed to participate in the study, including a manifest refraction and Stratus OCT (Zeiss) of the macula in each eye [11,12]. Any patients noted to have reduced vision with macular thickening were placed on a prolonged course of prednisolone acetate 1% (Pred Forte, Allergan) ketorolac 0.5% (Acular, Allergan), four times daily or bromfenac sodium 0.09% (Xibrom; Ista Pharmaceuticals, Irvine, CA, USA) twice daily for 1 additional month, and macular OCT was repeated monthly until resolution of CME or a decrease in macular thickness to normal was noted.
Results
One hundred thirty-five patients agreed to participate in the study and completed all follow-up visits. In total, 170 eyes (64 male and 106 female) qualified for the study. The average age was 70 years, with a range from 42 to 92 years. Eyes were excluded if they experienced iris trauma during the procedure or if they had any known disease other than cataract. The preoperative mean minimal foveal thickness was 185 ┬Ąm with a standard deviation of +/ŌłÆ15 ┬Ąm. Intraocular lenses included Crystalens 5.0, Crystalens HD, Rezoom, Restore, and aspheric acrylic new technology intraocular lenses. The average follow-up was 12 months with a range from 9 to 16 months.
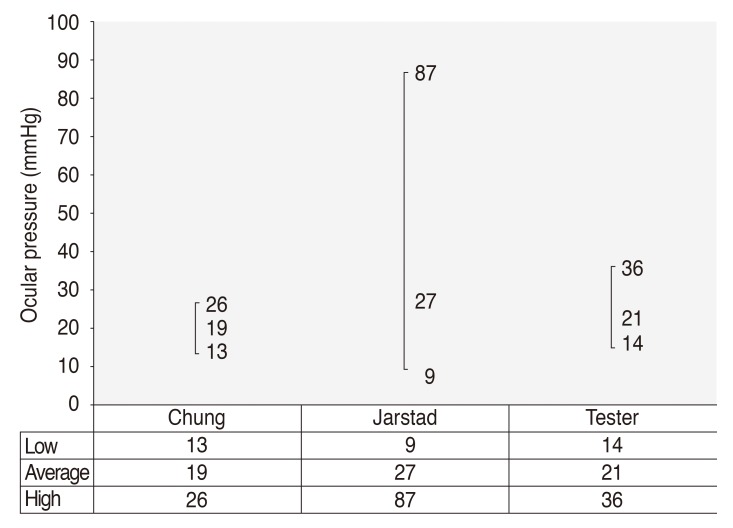
Immediate unadjusted postoperative IOP ranged from 9 mmHg to 87 mmHg as measured following what was deemed by the operating surgeon to be a ŌĆ£safeŌĆØ adjusted IOP on the operating table after the ophthalmic viscoelastic device material was removed mechanically with the irrigation/aspiration tip and the eye was refilled with balanced salt solution. A Weck spear was used to press on the eye to determine the appearance of an indent-able ŌĆ£safeŌĆØ pressure, and the watertightness of the MICS phaco wound was verified. The patient confirmed the ability to visualize the operating microscope light filament, and the IOP was tested with a TonoPen (AO Reichert) using a sterile cover.
Discussion
Prediction of immediate postoperative IOP varies greatly based on the surgeon and, in the present study, was initially not accurate (Fig. 1). We believe that scleral rigidity, increased elasticity in highly myopic patients, and decreased elasticity in hyperopic or older patients led to erroneously high or low estimates in the immediate postoperative IOP estimation [11]. Using the immediate feedback from the TonoPen measurements while the patient was still on the operating table, we were able to significantly improve predicted postoperative IOP with experience of two to three operating sessions (30 to 50 patients).
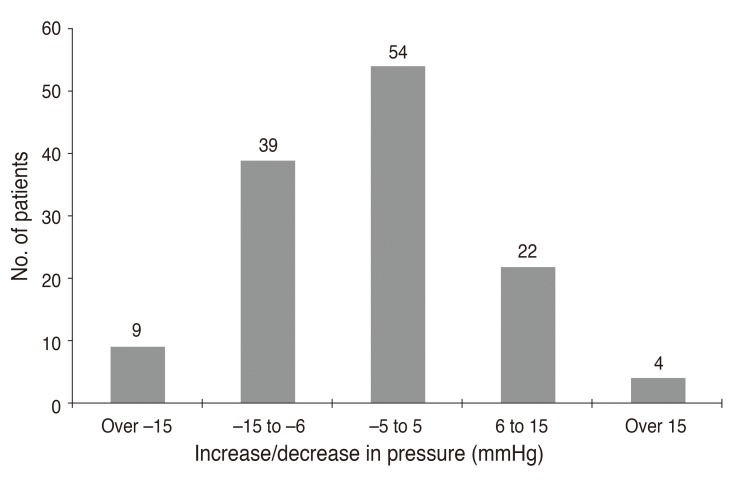
An additional finding was that the IOP varied only slightly from the final adjusted value on the operating table to that measured 24 hours later (Fig. 2). This seems to contradict other reported studies [15,16]. RF Brubaker, MD, at the Mayo Clinic (Rochester, MN) stated (September 1987) that the cause of a postoperatively elevated IOP ŌĆ£was unknown, since IOP was found to be elevated on postoperative examination the day following uncomplicated cataract surgery even before viscoelastics (ophthalmic viscoelastic device's) were introduced.ŌĆØ Our study, however, suggests that the IOP at the conclusion of the MICS cataract procedure is nearly the same as that measured at the day one postoperative exam.
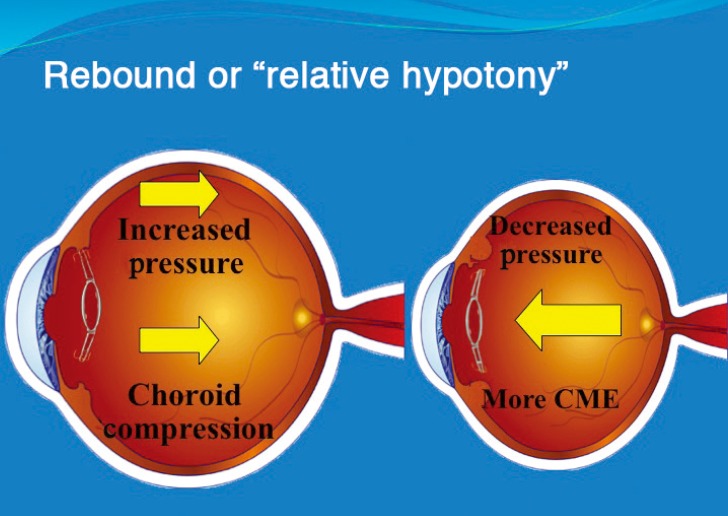
The macular OCT measurements conducted at 2 weeks are shown in Fig. 3. We found that patients with an IOP less than 16 mmHg had a four times greater incidence of CME compared to the control group with 16 mmHg to 21 mmHg (p = 0.012). Patients who had an initial postoperative pressure higher than 21 mmHg were noted to have a 2.5 times greater incidence of macular thickening (p = 0.029). We also confirmed that eyes with an extremely high initial IOP that was immediately adjusted to a safe range were more likely to develop macular thickening possibly due to ŌĆ£decompression retinopathyŌĆØ or ŌĆ£relative hypotony (Fig. 4),ŌĆØ as previously described by Bui et al. [17].
In conclusion, immediate adjustment of postoperative IOP on the operating table at the conclusion of cataract surgery may have a profound effect on preventing development of CME. Additionally, given very little change in IOP from the operating room table to the 1 day postoperative visit, we believe it is imperative to measure IOP immediately following completion of the cataract procedure in the operating theater or to become proficient with a tonometer in order to assure a safe pressure at the conclusion of surgery. The practice of immediate adjustment of postoperative IOP in the operating theater can provide an additional level of safety [18,19] to high-risk glaucoma patients undergoing cataract surgery [20] and to diabetic patients or those with compromised retinal vasculature, who are at higher risk for postoperative pressure spikes after anterior segment surgery [17,19,20,21,22].
Cost savings will result from fewer adjustments of IOP in patients who show unacceptable IOP spikes the day after surgery, who will no longer need tapping of the incision to a lower IOP, pressure-lowering medications, or additional eye drops. In our study, the additional time and expense of placing a lid speculum, tapping the incision with a sterile cannula, and repeat IOP testing if extrapolated over 1 year would cost approximately 44,000 dollars in lost physician and staff time and supplies necessary to adjust elevated postoperative IOP outside of the operating theater in a typical number of cataract patients according to the industrial engineer (KA Boudreau, MS, personal communication, January 2010).
Further studies are recommended to determine whether patient-specific matching of preoperative and postoperative IOP to individual eyes or evaluating whether high pressure phaco systems or excessive irrigating bottle height and relative decompression affect the blood retina barrier and lead to greater occurrence of CME. Micro incision cataract surgery in the future may include continuous control IOP monitoring and adjustment by biosensor feedback or implantable IOP-regulating transducers incorporated into the next-generation phaco systems to reduce the incidence of decompression retinopathy and associated CME.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






