Bilateral Branch Occlusive Retinal Vasculitis Induced by Septic Embo-lism in Endogenous Klebsiella Endo-phthalmitis
Article information
Dear Editor,
Endogenous Klebsiella endophthalmitis (KE) is usually fulminant and associated with high rates of evisceration and enucleation [1]. This report describes the first case of a patient with bilateral hemorrhagic occlusive vasculitis mimicking branch retinal artery occlusion as a complication of nephrogenic KE.
A 50-year-old woman with a history of type 2 diabetes mellitus was transferred to Asan Medical Center to manage Klebsiella bacteremia with multiple abscesses in her left kidney. As she reported painless blurred vision, the ophthalmologic service was consulted.
Her visual acuity was 20 / 32 in her right eye and 20 / 100 in her left eye. Slit lamp examination revealed moderate inflammations in the anterior chambers, but hypopyon was absent. Obliterative periarteritis surrounded by multiple retinal hemorrhages appeared in the infero-temporal artery of her right eye (Fig. 1A). Localized severe vitritis with hemorrhage was observed in the supero-temporal area and posterior pole in her left eye (Fig. 1B). Aspirated aqueous humor from both eyes was promptly cultured, and ceftazidime (2.25 mg/0.1 mL) and amikacin (0.4 mg/0.1 mL) were intravitreally administered to both eyes.
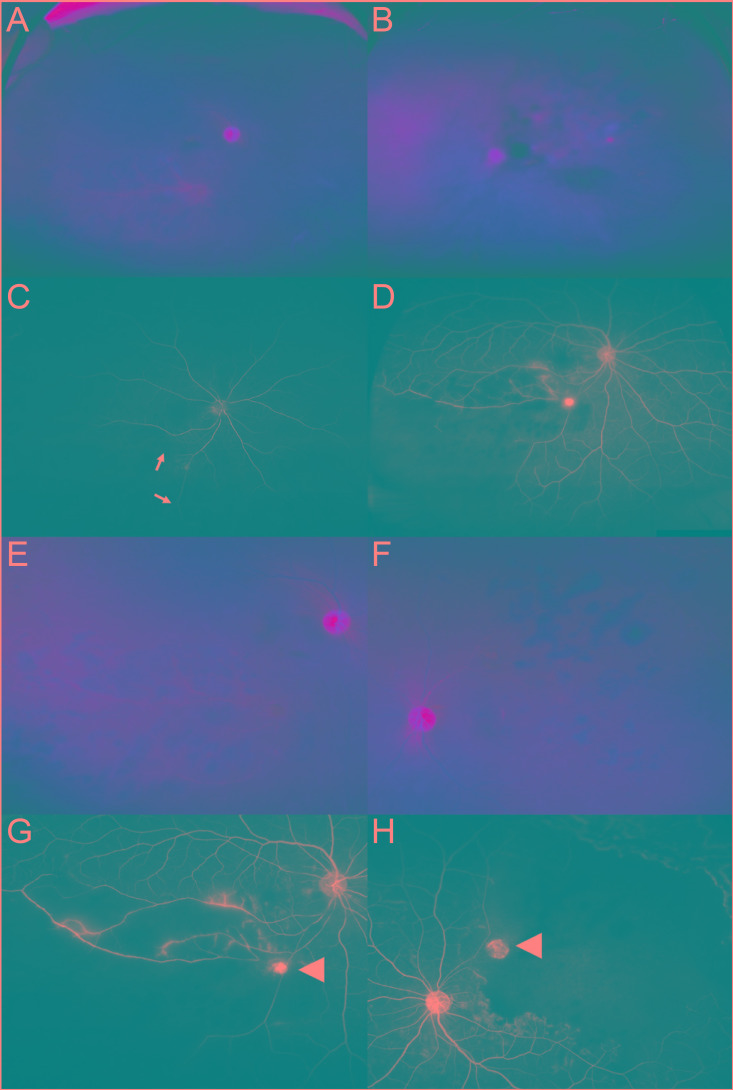
(A-D) Before treatment. (E-H) After treatment. (A) Wide-angle fundus photograph of the right eye, showing occlusion of the infero-temporal branch of the retinal artery and severe periarteritis, with multiple retinal hemorrhages. A round greenish lesion was observed at the first bifurcation site of the infero-temporal artery. (B) Wide-angle fundus photograph of the left eye, showing a similar hemorrhagic lesion in the supero-temporal peripheral area and localized severe vitritis in the posterior pole. (C) Fluorescein angiography (arterial phase) of the right eye showing delayed filling of the infero-temporal branch of the retinal artery (white arrows). (D) Fluorescein angiography (recirculation phase) of the right eye showing a sectoral pattern of non-perfused area with a round hyperfluorescent lesion in the angular point. (E) Fundus photograph of the right eye showing decreased retinal hemorrhage after treatment. (F) Fundus photograph of the left eye showing absence of vitreous opacity after vitrectomy. (G,H) Fluorescein angiography (recirculation phase) of both eyes showing extensive non-perfused area and hyperfluorescent emboli (arrow heads).
Fluorescein angiography of her right eye showed a sectoral pattern of non-perfused area due to infero-temporal arterial occlusion, as well as a round-shaped hyperfluorescent chorioretinal infiltration at the first bifurcation site of the infero-temporal major vascular arcade (Fig. 1C and 1D). Fluorescein angiography of her left eye showed diffuse vascular staining and blocked fluorescence caused by vitritis.
Because visual acuity and vitreal opacity in her left eye had worsened despite antibiotic injection, a vitrectomy was performed (Fig. 1E and 1F). Microbiologic cultures from aqueous and vitreous humor specimens were all negative. Angiography following the vitrectomy revealed supero-temporal non-perfusion involving the macular area in her left eye, along with another hyperfluorescent lesion at the first bifurcation site of the involved vessel, similar to her fellow eye (Fig. 1G and 1H). Her final visual acuity was 20 / 20 in her right eye and 20 / 160 in her left eye, the latter due to macular ischemia. Areas of non-perfusion in both eyes were treated with scatter laser photocoagulation.
Although the classic features of KE include decreased vision, injection, anterior chamber inflammation, and vitritis, retinal vascular involvement has also been reported [23]. For example, bilateral central retinal artery occlusions in a patient with hepatic KE were thought to be caused by a localized vasospasm under devastating conditions [2]. Similarly, extensive vasculitis in a patient with prostatic KE was thought to be associated with septic emboli in the retinal venule [3]. Although these reports yielded findings similar to ours, actual vascular flow was not assessed angiographically because of hazy media and poor patient general condition.
The patient described here exhibited relatively mild vitritis and a localized lesion, enabling the latter to be clearly evaluated by ultra-wide field fluorescein angiography. This method showed complete obstruction or delay in filling of the branch artery, which was identified as an attenuated vessel in the fundus. Moreover, a round hyperfluorescent lesion was identified near the bifurcation site of the attenuated branch artery, but branch retinal veins were not observed within the affected area. Hemorrhagic foci were scattered throughout the extensive non-perfused area, which was located around and distal to the round infiltration. These funduscopic and angiographic findings suggested that the round infiltration was a septic embolus, which could flow into the retina through the attenuated branch artery and cause extensive occlusive vasculitis around and distal to the emboli.
Septic emboli could gain access to the retinal circulation though septicemia, enabling them to lodge at the bifurcation site. An in vitro study showed that Klebsiella pneumoniae could attach to the endothelial surface and induce inflammatory responses in the blood-retina barrier [4]. These reactions may increase vascular permeability, which should be maximized in diabetic patients because of pericyte loss. Bacteria that invade the retina may release various proinflammatory and toxic compounds, which could directly stimulate leukocyte invasion and contribute to regionally devastating vascular reactions, including vasospasm and vasculitis near the infection focus.
To our knowledge, this is the first case of angiographically proven sectoral occlusive vasculitis associated with KE-induced septic emboli in both eyes. Patients infected with Klebsiella pneumoniae should undergo routine ophthalmologic screening, because subclinical vascular occlusion can occur and may leave behind sequelae which require further treatment even after controlling infection.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.