

Child abuse or maltreatment constitutes all forms of physical and/or emotional ill-treatment, sexual abuse, neglect or negligent treatment, or commercial or other exploitation that results in actual or potential harm to the child's health, survival, development, or dignity in the context of a relationship of responsibility, trust, or power [1]. Physical abuse of a child is that which results in actual or potential physical harm from an interaction or lack of an interaction, which is reasonably ŌĆ£a single or repeated incidentŌĆØ according to Child Welfare Information Gateway [2]. Harley [3] said that child abuse can also simply describe a battered baby, a physically abused child or an injury from a non-accidental trauma.
The United Nations Children's Fund (UNICEF)'s definition of child labor considers the fact that child labor seems to symbolize child abuse: in its explanations about child labor, UNICEF said ŌĆ£child labor describes the percentage of children aged 5 to 14 years involved in child labor activities at the moment of the survey. A child is considered to be involved in child labor activities under the following classification: (1) children 5 to 11 years of age that during the week preceding the survey did at least 1 hour of economic activity or at least 28 hours of one domestic work and (2) children 12 to 14 years of age that during the week preceding the survey did at least 14 hours of economic activity or at least 42 hours of economic activity and domestic work combined [4].ŌĆØ
Chana and Klauss [5] inferred that in developing countries, children may account for 40% to 50% of the total population. Yet, they are conspicuously neglected when national eye health and rehabilitation programs are planned. Most strategies are aimed at the adult age group instead of at children.
In Africa and other developing countries, the region's culture, traditions, and beliefs usually promote child abuse since acts of physical abuse can be seen as disciplining a child according to Abolfotouh et al. [6], Smith and Mosby [7], and Alyahri and Goodman [8] rather than being criminal by Committee on the Rights of the Child [9]. Previous studies have documented that ocular injuries may occur as a result of these practices [10,11,12].
There is a crucial need for this study as there is no known report in West Africa on ocular manifestations following child abuse in this population. Awareness therefore needs to be raised using facts on the potential eye injuries that could follow different forms of child abuse. Preventive measures should also be advocated.
Materials and Methods
A 2-year prospective descriptive study of consecutive cases of eye disorders that presented to an eye clinic following a history suggestive of child abuse was carried out between January 2012 and January 2014. Children between the ages of 0 to 16 years who visited the outpatient eye clinic were included. The study excluded any patients who were 17 years old and above. The diagnostic criteria for child abuse consisted of ŌĆ£any child presenting with a history of injuries sustained to the eye from beatings, maltreatment, child labor, hawking, and other related acts. ŌĆØ Socio-demographic characteristics, such as age, gender and parents' occupation, were also obtained. Presenting and posttreatment visual acuities were assessed according to the World Health Organization [13] classification of visual impairment.
The presenting visual acuity was obtained using illuminated Snellen charts read from a distance of 6 m, with one eye being examined at a time. Anterior segments were examined first with a bright penlight to quickly assess the injury sustained and thereafter with a slit lamp biomicroscope for a more detailed examination. Posterior segments and dilated fundal examination with a binocular indirect ophthalmoscope were also carried out to identify any changes in the lens (such as its position and if it was cataractous), the presence of vitreous changes and/or the observation of hemorrhages, exudates and traction. A +78 D lens was used to determine the cup-to-disc ratio. Other areas of the retina were assessed for hemorrhages, tears, or retinal detachment.
Intraocular pressures were also checked using Goldman's applanation tonometer where possible. When there was a rupture or an extensive globe laceration, digital tonometry was conducted to determine whether the globe was soft (hypotony or low intraocular pressures) or not.
Ocular ultrasound was also undertaken to confirm some conditions, such as a collapsed anterior chamber, cataracts, vitreous opacities, and retinal detachments. All cases that required surgical repair were treated except for cases with retinal detachment, which had to be referred to the vitreo-retinal surgeon at another center.
Results
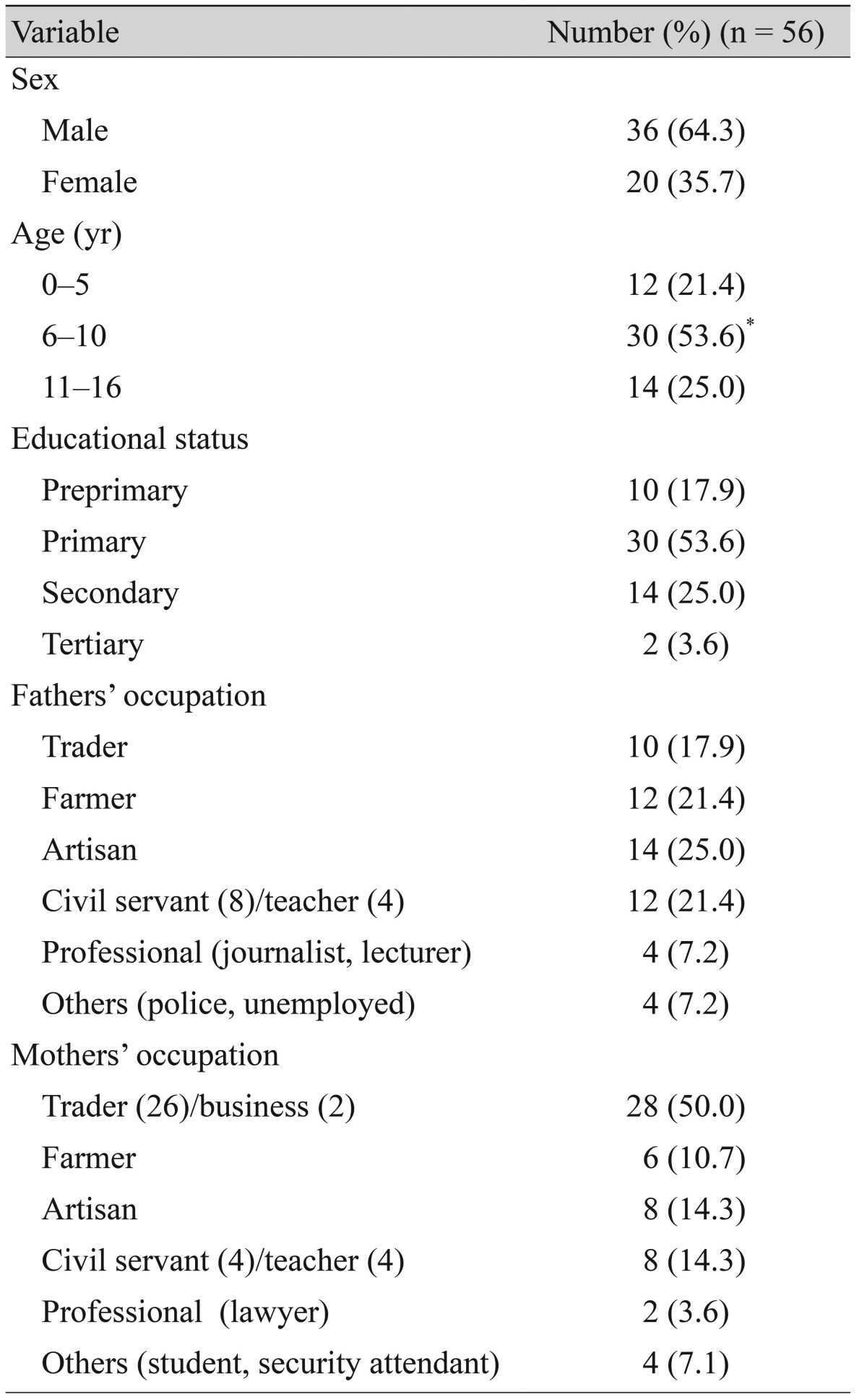
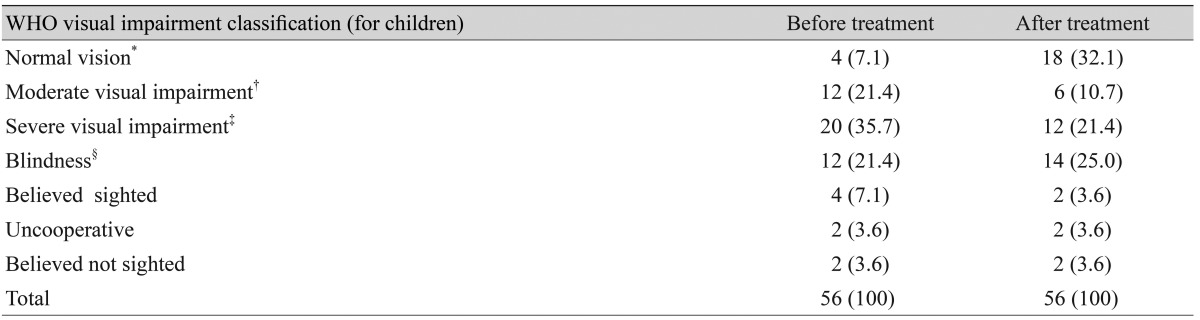
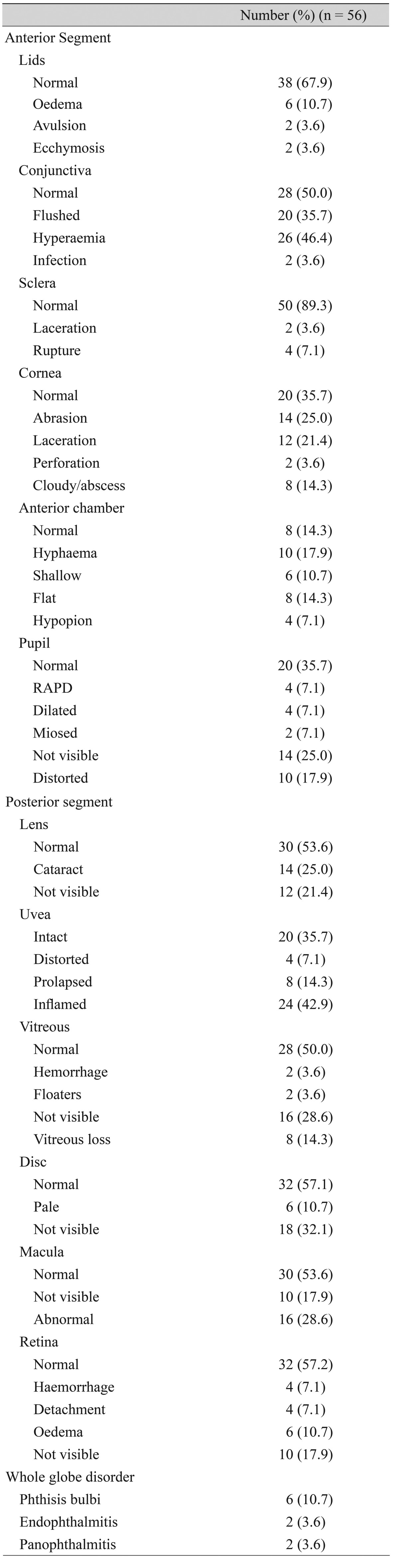
Fifty-six eyes of 56 children were examined. There were 36 males (64.3%) and 20 females (35.7%). The participants' ages ranged from 2 to 16 years with a mean age of 8.25 ┬▒ 3.55 years, while the modal age group was 6 to 10 years (standard deviation, 0.68). Primary school children predominated, as there were 30 (53.6%) in this study, while the remaining 26 (46.4%) were secondary school students and others (Table 1). The proportion of affected eyes (39.3%) included 36 right eyes (64.3%) and 20 left eyes (35.7%). Presenting versus posttreatment visual acuities are shown in Table 2. The distribution of common ocular disorders were conjunctiva hyperemia (46.4%), corneal abrasion/ulcers (25.4%), anterior uveitis (42.9%), and cataracts (25.0%), as shown in Table 3.
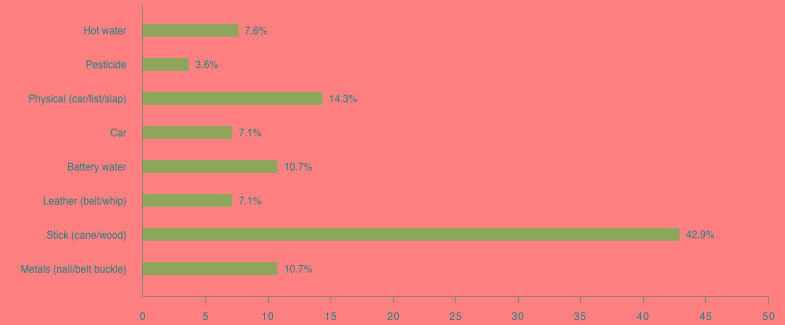
Fig. 1 indicates the most commonly injurious agents were canes (25.0%) and sticks (17.9%). The distribution of persons who inflicted the injuries is shown in Fig. 2. The circumstances that led to the events mostly followed child labor in 22 participants (39.3%) or physical beatings in 14 cases (25.0%). Corporal punishment or assault each were responsible for injuries in eight cases (14.3%) that were closely followed (Table 4). Common complications included those affecting the eye lids (two mechanical ptosis cases and two notched margins), which were identified in four total eyes (7.1%). For the cornea, 14 cases had opacity, four presented with adherent leukoma, two suffered from descemetocoeles, and two exhibited siderosis, totaling 22 eyes (39.3% of the sample). For globe injuries, there were six cases of phthisis bulbi, two panophthalmitis reports and two endophthalmitis cases in a total of 10 eyes (17.5%). Occlusio pupillae was present in one participant, while 14 eyes had cataracts (25%), and four suffered from retinal detachment (7.1%).
The globe was intact in 38 eyes (67.9%) in our sample of patients. Only six children (10.5%) experienced no complications. Intraocular pressures were normal in 14 (25.0%), elevated in 10 (17.9%), and difficult to assess in 32 eyes (57.1%).
Discussion
Child abuse is usually not considered a ŌĆ£sinŌĆØ against children in Nigeria because the cultural environment seems to favor child labor, which is usually associated with child abuse. This study has revealed that males were 1.5 times more affected than females. This trend likely reflects the tendency for males to be more daring and aggressive in acts or attitudes while being sent on an errand. Males are also known to be more stubborn, and they are more likely to become involved in rough play than the girls according to Shumba [14]. These tendencies seem to predispose males to accidents and injuries as well as ŌĆ£punishment, ŌĆØ which is supposed to be a deterrent but instead could lead to abuse of the child.
The age group from 6 to 10 years was observed to have the highest number of affected eyes. This is the age bracket when children are more likely to be sent on errands, where they can either sustain ocular injuries from accidents or be subject to abuse. This age group corresponds to the primary school age. These are very young children who do not deserve to be treated in a way that can negatively affect their vision. The consequences are reflected in the visual acuity status (Table 2); two children became blind due to complications from abuse in this study. Fortunately, a high number regained normal vision or experienced improvement with treatment.
Most of the children's fathers were artisans, farmers and traders, while their mothers were mainly traders. Oyedeji [15] suggested that due to the parents' low education levels, these children would likely fall into a low socio-economic group. This low status may explain why these children or wards are more affected than the children in higher socio-economic groups. Because the children are not adequately provided for, they therefore have a tendency to go hawking on the streets in order to contribute to the family's maintenance.
We found various types of ocular abnormalities in our study. For example, different types of lid abnormalities, such as edema, ecchymosis and avulsion, were observed (Table 3). These have also been identified in East Africa, where avulsion is commonly a result of sexual assault according to Chana and Klauss [5]. Sexual assault was, however, not recorded in our study. In the anterior segment, red eyes, corneal and pupillary lesions, and hyphema were seen. These conditions are highly correlated with trauma to the eyes, which could be sustained from blunt objects, fists, canes, and sticks. The sharp edges of metal objects like belt buckles, which constituted 10.7% of the injurious agents in this study, can also cause scleral rupture or corneal laceration. Two cases of globe rupture had been previously reported for the first time in an infant and a 14-month-old child in New Mexico, United States of America by Skarbek-Borowska and Campbell [16].
In posterior segment cataracts, the observed vitreous and retinal lesions result from the force of trauma to the eyes. There are also entire globe disorders that produce panophthalmitis and endophthalmitis. These conditions are the sequelae of infections to the eyeball that follow an open globe injury. They have a poor prognosis and usually lead to blindness. After these two conditions occur, the eyeball may end up being shrunken, which usually poses a cosmetic problem for the individual. In a child, a shrunken eyeball not only provides a poor cosmetic appearance but also hinders proportionate facial and orbital bone development [17].
The types of eye injuries reported in developed countries appear to differ from those that are seen in developing countries. In the former, features of retinal hemorrhages and shaken baby syndrome appear to almost always be synonymous with child abuse. Studies carried out by DeRidder et al. [18], Matschke et al. [19], and Levine [20] found that these are usually reported early in infancy or in children under the age of 5 years. However, in developing countries, resultant injuries from physical abuse and corporal punishment appear to be the same as those seen in Nigeria, as similar reports have been published in Jamaica, Egypt, and Yemen [6,7,8]. Death could also accompany the retinal features, since they are an offshoot of brain injury. The level and extent of the injury sustained could also be determined by the use of modern investigative methods, including diffusion-weighted magnetic resonance imaging, which can identify retinal ischemia and hypoxia according to Blumenthal [21]. Death has also been reported in Nigeria by a lawyer following severe injuries sustained from corporal punishment [22]. Recently, features of subconjunctival hemorrhages have been reported to occur in child abuse cases. These hemorrhages should also be watched for in babies or in cases with non-accidental head trauma [22].
It should be noted that cases of child abuse were not seen among babies or infants in this study. This trend may have been coincidental. Another study on babies and infants that can be conducted at pediatric outpatient and infant welfare clinics may be needed to compare the findings.
Among the perpetrators of child abuse, relatives, self-injuries and teachers/household helpers topped the list in descending order. This trend of the perpetrators being relatives of the victim is similar to the findings of studies carried out in Jamaica, where parental violence is the most commonly reported kind of family physical violence [7]. This type of behavior also holds true in most Nigerian cultures because it is believed that ŌĆ£if you spare the rod, you spoil the child, ŌĆØ which could taint the family name and image.
In Alexandria, Egypt, 76.3% of children in the fifth grade who were surveyed had been corporally punished according to Smith and Mosby [7]. It is interesting to note that the role of teachers in inflicting physical injury through corporal punishment was much lower in this study (10.7%) as compared to a study from Zimbabwe, where trained teachers were observed to contribute about 92.0% of physical abuse through corporal punishment of pupils in primary schools in the form of pinching, whipping, punching, and kicking. However, that study was conducted among teachers in the schools, which explains the high prevalence of reported cases by Shumba [14]. The low percentage identified in the present study could be a sign of a declining trend of the use of corporal punishment by teachers in schools in Southwest Nigeria. These teachers probably believe that ŌĆ£charity begins at home, ŌĆØ so the parents should really take charge of their children's moral training instead of teachers. A survey conducted among Nigerian primary school teachers by Mahmoud et al. [23] revealed that a majority of the body sites used during punishment involved the buttocks (61%) and a hand, while the face was the least (28.0% of cases) common. Being beaten up also constituted the same proportion as corporal punishment (25.0%). Oftentimes, the act was perpetrated by family members.
Self-injuries were the third commonest method by which persons sustained eye injuries in our present study. These accidents happened to children who were either sent out street hawking, where they either fell down or into a ditch or were knocked down by an automobile, or they were injured when left alone at home to fend for themselves or with uncaring house help. The most common injurious agents involved were the stick (cane/wood) (42.9%), followed by physical agents such as the hand/fist/slap (14.3%).
These results seem to corroborate the finding that the types of punishment often meted out are mainly physical, which may produce eye injuries. The authors hereby advise other forms of punishment, such as taking away toys, privileges or time spent watching TV. Rescinding privileges was reported in Zimbabwe to constitute 39.3% of punishment for children [14]. In Yemen, more than half of rural and about a quarter of urban caregivers meted out harsh corporal punishment in the form of using objects, biting or pinching. It appears that in developing countries, corporal punishment is rampant.
In many cases, the circumstances that led to the child being abused occurred when the child was being beaten up (25.0%) or being used for child labor (39.3%). During child labor, these children are made to do the work of an adult. For example, some are forced to become an apprentice instead of attending school, or to cook and take care of another child or to trade. These types of labor are related with the types of injurious agents. For example, battery acid caused chemical injuries to the eyes of two children who were apprentice mechanics, while hot water caused thermal burns in another. Of course, hawking on the streets also predisposes the child to automobile and other types of road accidents.
Child neglect is also another contributory factor. Due to economic recession, parents may leave their children at home in the care of another child. Inexperience could lead to home accidents, such as those recorded in this study where pesticides (3.6%) and hot water (7.6%), caused ocular injuries. Similarly, in East Africa, children sustained hot water burns when pouring a boiling pot of water [5].
Negative side effects, such as poor performance in school, have been reported following ocular injuries in Zimbabwe and Yemen; therefore, corporal punishment should be discouraged [8,14]. However, side effects and psychosocial abnormalities were not investigated in our study. These topics could be explored in future studies.
Families of children who are victims of child abuse should be thoroughly investigated by child right agencies. Unfortunately, laws that protect children in Nigeria are still deficient, especially after the United Nations Conventions on the Rights of the Child were ratified. Everyone in this society is therefore enjoined to be vigilant and report likely or suspicious circumstances to law enforcement agencies to reduce ocular morbidity and child mortality from cases of child abuse [22]. Knox [24] made an appeal in the United States of America by some authors to better educate and make parents aware of child maltreatment, which will ultimately reduce the incidence of abusive ocular injuries.
In conclusion, after treatment, the proportion of visual impairments increased, while that of blindness significantly decreased. Legislation needs to be developed and laws must be effectively put in place to prevent these occurrences, which could negatively impact the psychological, social and economic wellbeing of the child, family and country as a whole.


 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






