

Dear Editor,
Mirror-image twinning with inverse laterality happens in 10% to 15% of monozygotic twins and can be useful in establishing that twinning events have occurred after the cells of the embryonic plate began to lateralize, but before formation of the primitive streak [1]. Previous reports on ocular mirror image included cases with myopic anisometropia, infantile esotropia, infantile nystagmus, optic glioma, optic nerve dysplasia, and retinoblastoma [2,3]. Herein we report a case of monozygotic twins with mirror-image myopic anisometropia who developed ocular myasthenia gravis (MG) and had remnant motility defects in mirror-image eyes. To the best of our knowledge, this is the first report of ocular MG in mirror-image twins.
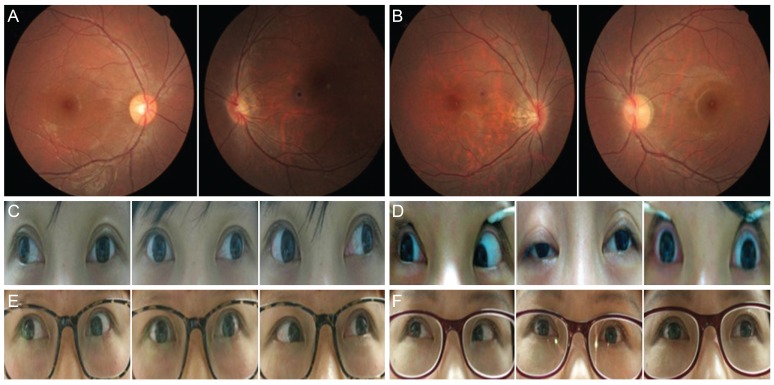
A pair of 26-year-old female twins presented with mirror-image asymmetry of monocular low vision and motility deficits. One (twin 1) had myopic anisometropia, a myopic disc, and an adduction deficit in the left eye, while the other (twin 2) exhibited the same conditions in the right eye.
Anisometropia of -0.75 Dsph -1.00 Dcyl axis 90 (20 / 20) in the right eye and of -6.50 Dsph -1.50 Dcyl axis 90 (counting fingers) in the left eye, whereas the same measures for twin 2 were -8.00 Dsph -1.50 Dcyl axis 180 (counting fingers) in the right eye and -5.00 Dsph -1.50 Dcyl axis 180 (20 / 25) in the left eye. On fundus examination, a myopic tilted disc with parapapillary atrophy and tigroid fundus with reduction of the foveal reflex were observed in the left eye of twin 1 (Fig. 1A) and in the right eye of twin 2 (Fig. 1B).
These twins had a history of ocular motility disturbances and a positive acetylcholine receptor antibody titer, which led to a presumptive diagnosis of ocular MG. They had previously had an eye examination at 19 years of age. On this initial examination, twin 1 exhibited left exotropia of 55 prism diopters and limited adduction in both eyes, which was more marked in the left eye (Fig. 1C). She stated that this problem was first noted at 4 years of age, but she did not complain of diplopia. Twin 2 exhibited fluctuating ptosis and various motility deficits, which had been more prominent in the right eye 1 year prior (Fig. 1D). The results of anti-acetylcholine receptor binding antibody test were weakly positive (>0.200 nmol/L; 0.282 nmol/L for twin 1 and 0.227 nmol/L for twin 2). Twin 2 was administered a combination of pyridostigmine and methylprednisolone, which was decreased gradually over a 2-year period. This medication led to complete normalization of acetylcholine receptor antibody titer, resolution of ptosis, and stabilization of motility disturbances. The patients had no speech or swallowing problems or limb girdle weakness during 2 years of follow-up.
At the recent examination (7 years after initial visit), twin 1 was orthotropic with a -2 limitation of adduction in the left eye (Fig. 1E). She underwent muscle surgery for left exotropia at other clinics 2 years ago. Twin 2 had right exotropia of 25 prism diopters and a -4 deficit of adduction in the right eye (Fig. 1F). With the exception of ocular abnormalities, they were generally healthy and on no other medications.
Our patients showed a prominent remnant inability to adduct each eye with mirror-image myopic anisometropia. MG is a heterogeneous and complex disorder, but there is strong evidence that an individual's genetic make-up is an important predisposing factor for its development [4]. In addition, there are a number of case reports describing the concordance of generalized MG in monozygotic twins in terms of neurology and/or immunology. Furthermore, Punga et al. [5] reported a case of monozygotic twins with neuromuscular transmission defects at opposite sides of the motor end plates: MG and Lambert-Eaton myasthenic syndrome. Therefore, a possible explanation for mirror-image twinning of ocular MG is that anatomic similarities within the neuromuscular junction of extraocular muscles lead to a similar predisposition to MG. The addition of our report to the literature implicates a strong underlying genetic susceptibility in the pathogenesis of MG.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






