Successful Treatment with Chronic Conjunctivitis: Removal of Tarsoconjunctival Crypt
Article information
Dear Editor,
Contrary to the majority of acute conjunctivitis cases, chronic conjunctivitis can be caused by infection or inflammation of the lacrimal duct system, conjunctival intraepithelial neoplasm, floppy eyelid syndrome, and immunologic reaction [12]. Symptoms are presented as insidious discharge, eye redness, and foreign body sensation. Chronic conjunctivitis is usually not self-limited. Some cases of antibiotic-resistant chronic conjunctivitis in conjunction with tarsoconjunctival crypts have been reported [3]. A thorough marsupialization of the crypts and short-term treatment with antibiotic eye drops can prevent recurrence. In this article, we report a patient with a similar form of chronic conjunctivitis that was refractory to multiple courses of antibiotic therapy.
A 40-year-old female patient was referred to Ilsan Paik hospital for ocular discomfort and conjunctival injection on the left eye. The patient had been experiencing discharge and conjunctival injection for 1 month. Her vision was 20 / 20 in both eyes. A slit lamp biomicroscopy revealed scarring in the left upper and lower tarsoconjunctival, multiple concretions, and subconjunctival fibrosis (Fig. 1A). Topical therapies including gatifloxacin ophthalmic solution 0.3% and prednisolone acetate 1% were attempted but failed to resolve her symptoms. Culture of the discharge revealed Pseudomonas aeruginosa. We prescribed additional therapies of moxifloxacin, tobramycin ophthalmic solution, and oral doxycycline. Exposed concretions were removed twice, but her symptoms were not resolved. Two weeks after the original admission, right ocular discomfort was noted. We prescribed the same eye drops for her right eye as for the left eye. After 1 month of treatment and no change in symptoms, we decided to remove the tarsoconjunctival fibrosis of both eyes. The anatomic findings were similar in both upper eyelids (Fig. 1A and 1B). To determine the full extent of the conjunctival tunnels on the epitarsal surface, a probe was passed through the fistulous opening (Fig. 1C). The patient underwent marsupialization of both upper eyelid tarsoconjunctival crypts (Fig. 1D). Many concretions under subconjunctival fibrosis were removed. Bacterial culture of squeezed concretions was conducted, and the results were the same as the earlier culture obtained from the discharge: Pseudomonas aeruginosa. After marsupialization of both upper eyelid tarsoconjunctival crypts, conjunctival injection had much improved, and the dense conjunctival fibrosis was decreased but still apparent (Fig. 1E and 1F). Her discomfort gradually resolved. One month after the procedure, although the conjunctival fibrosis remained, we discontinued her eye drop treatment and medication because her symptoms of foreign body sensation, erythema, and discharge had improved.
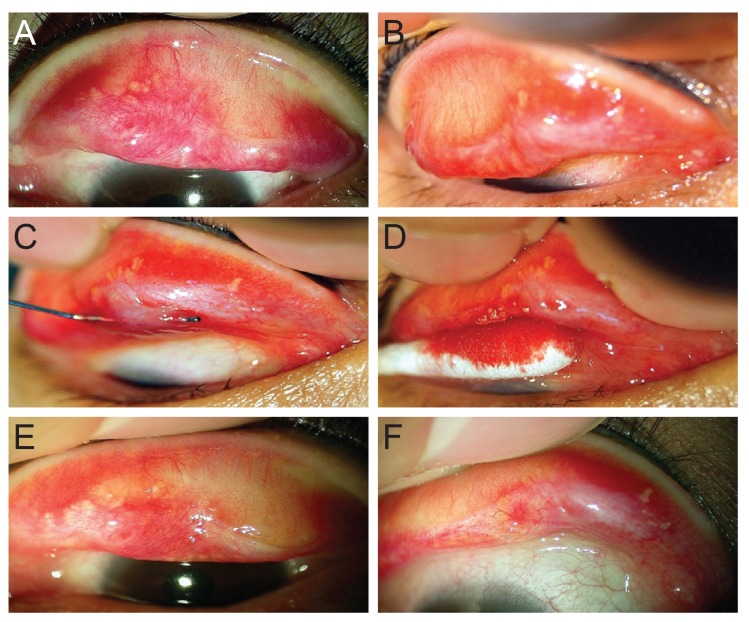
Photographs showing the everted upper eyelids of a 40-year-old woman with chronic conjunctivitis. (A) Left upper lid, eversion of the left upper eyelid reveals tarsoconjunctival scarring and multiple concretions. (B) Right upper lid, eversion of the right upper lid reveals a pseudomembrane on the medial tarsal conjunctival surface and subconjunctival fibrosis. (C) Right upper lid, a probe is passed through the fistulous opening to expose the full length of the tarsoconjunctival tract. (D) Right upper lid, squeezing of the tarsal plate expels multiple concretions through the exposed crypts. (E) Left upper lid, 1 month after the procedure, conjunctival injection is much improved, and the dense conjunctival fibrosis was decreased but still present. (F) Right upper lid, the same findings as for left tarsoconjunctiva.
Here, we reported a patient suffering from continuous eye discomfort refractory to oral antibiotics and antibiotic eye drops. Tse et al. [3] have reported three cases of chronic mucopurulent conjunctival discharge that were refractory to multiple courses of antibiotic therapy. In all the cases of the study, the subjects' symptoms were attributed to tarsoconjunctiva filled with coagulum and that was connected through fine fistula tracts. Based on these findings, Tse et al. [3] introduced the term 'tarsoconjunctival crypts.' They postulated that the tarsal conjunctiva sequestration of bacteria was initiated by trauma caused either by inflammation from Stevens-Johnson syndrome or by mechanical abrasion from nocturnal lid eversion. Partial sloughing of the tarsal conjunctiva and subsequent re-epithelization over a lamellar layer of epithelium formed an epithelized tunnel to trap the bacteria. Generally, chronic concretions do not need to be removed unless they are exposed, because their removal can aggravate other conjunctival and corneal surfaces. Unlike the cases in Tse et al. [3], our subject had no specific ophthalmologic conditions. Although patients reporting discomfort due to continuous discharge or conjunctival injection refractory to antibiotic eye drops might not have any other ocular disease, upper or lower eyelid eversion is necessary to treat relapsing mucopurulent conjunctivitis that does not respond to topical antibiotic eye drop treatment.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.