

Dear Editor,
Refractive surgeons have become interested in surface ablation because this procedure is free of flap complications, has less iatrogenic ectasia and yields better visual quality. Dealing with corneal haze after surgery, a potential complication of surface ablation, is very challenging for refractive surgeons [1]. Phototherapeutic keratectomy (PTK) is one option that may help some patients. However, with this procedure, postoperative vision is unpredictable because of refractive changes, usually hyperopic shifts after PTK [2].
We report our experience with two patients who developed subepithelial haze after surface ablation; both were successfully treated with PTK coupled with photorefractive keratectomy (PRK) with pre-PRK planning using intraoperative skiascopy.
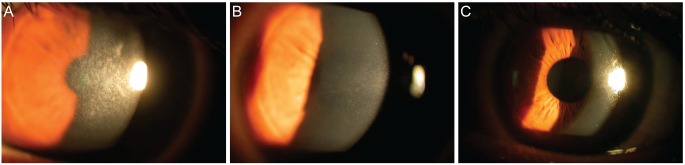
Case 1, a 22-year-old male patient was referred to an out-patient clinic for corneal haze after epi-laser in situ keratomileusis procedures on both eyes. The patient had been experiencing blurred vision at one month postoperatively, and was referred to our institution at three months postoperatively with progressive, gradual loss of visual acuity in both eyes. Vision was 20 / 200 (20 / 32 with -4.00 diopters [D] = -1.25 Dcyl 180┬░) in the right eye and 20 / 200 (20 / 40 with -4.50 D = -0.75 Dcyl 180┬░) in the left. Ultrasonic pachymetry measurements were 574 ┬Ąm in the right eye and 548 ┬Ąm in the left. Slit lamp biomicroscopy revealed dense subepithelial opacification in both eyes (Fig. 1A) with moderate obscuration (grade 3) of the iris and lens. We planned a combined therapy of PTK-PRK-mitomycin C soaking-amniotic membrane transplantation for removal of the left eye corneal haze. Transepithelial PTK (7.0-mm diameter, depth 82 mm) was performed using excimer laser (Z100; Bausch & Lomb Surgical, Rochester, NY, USA) until we observed the removal of the epithelium. After PTK, intraoperative skiascopy was performed in the operating room. Interestingly, the skiascope beam was clearly seen and the refraction was -3.00 D = -0.50 Dcyl 180┬░, which was different from the value obtained before PTK. PRK (6.0-mm diameter, depth 61 mm) was performed, guided by the intraoperative skiascopy data. After PRK, a merocel sponge soaked with mitomycin C 0.02% was placed over the cornea for 1 minute. Temporary amniotic membrane transplantation was performed. Topical Cravit and Pred Forte were each prescribed, four times daily for a month. One month after surgery, the identical procedure was performed on the right eye. Two months after left eye surgery, the subepithelial haze had almost disappeared and the corneal surface appeared stable (Fig. 1B). On last follow-up, 4 years after surgery, vision was 20 / 32 (20 / 20 with plano = -0.50 Dcyl 175┬░) in the right eye and 20 / 32 (20 / 20 with +0.50 D) in the left eye (Fig. 1C).
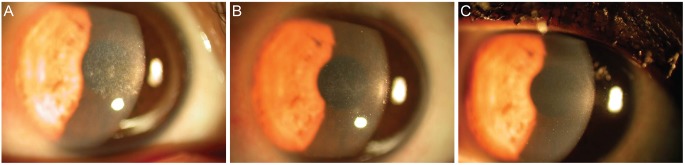
Case 2, a 27-year-old female patient was referred for corneal haze after laser-assisted subepithelial keratectomy. Three months postoperatively, subepithelial haze appeared in the right eye and became progressively worse. One year after laser-assisted subepithelial keratectomy, vision was 20 / 200 (20 / 20 with -1.75 D = -1.00 Dcyl 10┬░) in the right eye. Ultrasonic pachymetry measurement was 462 ┬Ąm in the right eye. Slit lamp biomicroscopy revealed a dense region of central subepithelial opacification in the right eye (Fig. 2A), with moderate obscuration (grade 3) of the iris and lens. The surgical procedure described above was performed. Two months postoperatively, the cornea appeared clear and the corneal surface seemed stable (Fig. 2B). At last follow-up 1 year after surgery, her vision was 20 / 20 (20 / 20 with -0.50 D) in the right eye (Fig. 2C).
To date, the exact mechanism of corneal haze development after surface ablation is uncertain. Regardless of the technique used, a key event after excimer photoablation is epithelial injury, which triggers cytokine release [3,4].
When basement membrane and Bowman's membrane are removed by surface ablation, the regenerated epithelium is supposed to be hyperplastic and adhere strongly to stroma. Therefore, manual debridement in management of corneal haze carries the risk of uneven stromal exposure. To address this problem, we conducted transepithelial PTK until the stroma was adequately exposed.
Although PTK has been reported to be effective in the management of superficial corneal haze and irregularity in many conditions, refractive changes and irregular ablation after PTK are frequently reported [5]. Patients who suffer complications after refractive surgery fully expect good uncorrected vision after retreatment. It is probable that unwanted refractive errors occur after PRK, considering the significant ablation depth of PTK.
Therefore, to avoid unwanted refractive changes after PTK, intraoperative skiascopy was performed with patients in the sitting position. We ablated the cornea with PRK; however, this procedure was guided by our measurements of adjusted refractive errors. Though we present data from only two patients, we suggest that this approach is unique to our practice and an effective means of both removing corneal haze and avoiding corneal irregularity and refractive error after retreatment.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






