Argon Green Laser for Valsalva Retinopathy Treatment and Long-term Follow-up of the Internal Limiting Membrane Changes in Optical Coherence Tomography
Article information
Dear Editor,
We experienced a case of sub-internal limiting membrane (ILM) hemorrhage successfully treated with an argon green laser (AGL) posterior hyaloidotomy. We could not identify any report in the ophthalmic literature describing spectral domain optic coherence tomography (OCT) localization of AGL spots or preoperative exact anatomic localization in valsalva retinopathy.
A 35-year-old man presented with sudden blurred vision in the right eye that occurred one day before examination. Dilated fundus examination of the right eye showed a well-circumscribed large sub-ILM hemorrhage in the temporal macular area (Fig. 1A). Fluid was noted in the upper part of the hemorrhage. OCT (Spectralis; Heidelberg Engineering, Heidelberg, Germany) revealed a dome-shaped hypo-reflective area, consistent with blood beneath a hyper-reflective band at the macula (Fig. 1B). OCT scans just above the level of sedimented blood revealed two distinct membranes overlying a preretinal hemorrhage. The membrane on the retinal side, more apparent and reflective, was identified as ILM. The slight and patchy overlying membrane was identified as posterior hyaloid, and a mild vitreous hemorrhage was noted (Fig. 1C). A dense preretinal hemorrhage produced shadowing that precluded analysis of the retina and subretinal space. We used AGL photocoagulation (Lightlas 532 Green Laser; Lightmed, San Clemente, CA, USA) to perforate the hyaloid and ILM in order to drain the sub-ILM blood into the vitreous cavity. Four exposures of AGL were performed at the inferior margin of the hematoma's anterior surface with a spot size of 100 µm, exposure duration of 0.1 seconds, and power of 200 mW. Patient informed consent was obtained. Consequently, the hemorrhage was rapidly drained inferiorly into the vitreous cavity (Fig. 1D). Fundus photography revealed strong resolution of the hemorrhage (Fig. 1E). OCT revealed laser perforation points along the ILM and hyaloid (Fig. 1F). The hyporeflective space between the ILM and the nerve fiber layer was possibly due to the presence of residual blood. In addition, blood in the vitreous cavity was still observable on the OCT (Fig. 1G). At a two-year follow-up visit, visual acuity was stable at 1.0, and the patient did not mention any symptoms of metamorphopsia. Although the hemorrhage was completely resolved (Fig. 1H), laser perforation points were incurred during the procedure, and a lamellar hole and failed reattachment of ILM were observed in the temporal macular area in the OCT at final follow-up (Fig. 1I). The OCT also revealed that the detached ILM had attached to the posterior hyaloid (Fig. 1J).
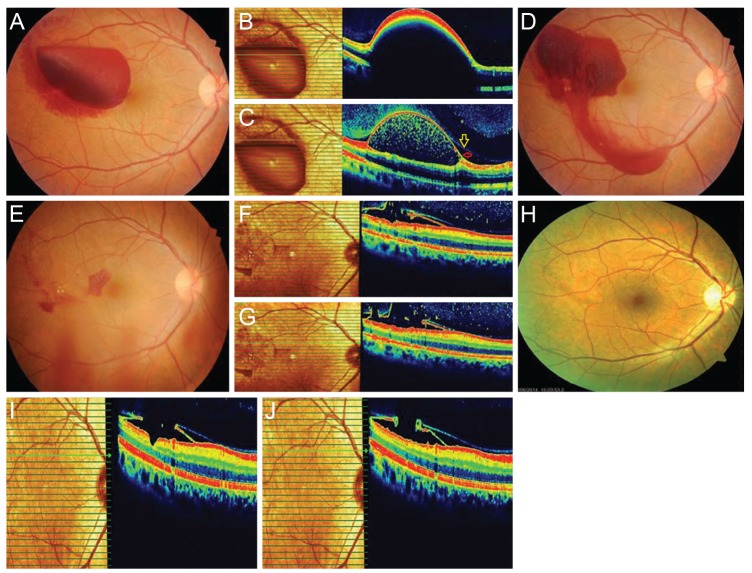
(A) Fundus photograph of the right eye showed a huge sub-internal limiting membrane (ILM) hemorrhage in the temporal macular area. (B) Spectral domain optic coherence tomography (OCT) revealed a dome-shaped hypo-reflective area, consistent with blood beneath a hyper-reflective band at the macula. (C) Spectral domain OCT reveals two distinct membranes: the more apparent and reflective one was identified as ILM (red arrow), and the other slight and patched membrane was identified as posterior hyaloid (yellow arrow). (D) The hemorrhage was drained inferiorly after the argon laser procedure. (E) Fundus photograph reveals strong resolution of the hemorrhage after three weeks. (F,G) OCT reveals laser perforation points along the ILM and hyaloid after three weeks. (H) There was no hemorrhage in fundus photograph after two years. (I) Pseudo-hole and no reattachment of ILM are observed in the temporal macular area in the last OCT. (J) OCT reveals that the detached ILM was attached to the posterior hyaloid and formation of no epiretinal membrane after two years.
The anatomical location of premacular hemorrhage, either under the ILM (sub-ILM) or subhyaloid, is still controversial and is not possible to distinguish using indirect fundus examination [12]. Intraoperative findings and time-domain and spectral domain OCT images in recent articles support previous histologic reports of premacular hemorrhage beneath the ILM in Valsalva retinopathy [3]. In the present case report, the sub-ILM location of the hemorrhage was confirmed in spectral domain OCT. Thus, in our opinion, valsalva retinopathy caused the sub-ILM hemorrhage. In this sense, the term subhyaloid hemorrhage is a misnomer. We think that the term sub-ILM hemorrhage should be used instead of subhyaloid hemorrhage.
According to our previous experience, Nd:YAG laser membranotomy requires relatively many spots with higher energy levels for the treatment of the premacular hemorrhage [4]. We used AGL with low energy to stretch the posterior hyaloid and the ILM. OCT revealed localization of the ILM and hyaloid membrane disruptions and attachment caused by the laser spots and the safety of the procedure, with minimal involvement of the underlying retinal layers after two years of follow-up. We punctured the posterior hyaloid face and ILM with an AGL in order to drain a premacular hemorrhage into the vitreous and to allow absorption of the blood in the vitreous space.
We concluded that spectral domain OCT evaluation of laser treatment for valsalva retinopathy can confirm the cleavage plane of a valsalva hemorrhage. In order to avoid retinal tissue damage, exact anatomical localization of hemorrhage was determined using spectral domain OCT. This method can also be used for follow-up after laser application. The treatment of AGL seems to be helpful in the rapid clearing of a premacular hemorrhage by causing disruption of the ILM. However, larger case studies are required to compare the effects of the different laser techniques.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.