Comparison of Surgical Outcomes with Unilateral Recession and Resection According to Angle of Deviation in Basic Intermittent Exotropia
Article information
Abstract
Purpose
The purpose of this study is to compare the surgical outcomes and near stereoacuities after unilateral medial rectus (MR) muscle resection and lateral rectus (LR) recession according to deviation angle in basic intermittent exotropia, X(T).
Methods
Ninety patients with basic type X(T) were included in this study. They underwent unilateral recession of the LR and resection of the MR and were followed postoperatively for at least 12 months. Patients were divided into three groups according to their preoperative deviation angle: group 1 ≤20 prism diopter (PD), 20 PD< group 2 <40 PD, and group 3 ≥40 PD. Surgical outcomes and near stereoacuities one year after surgery were evaluated. Surgical success was defined as having a deviation angle range within ±10 PD for both near and distance fixation.
Results
Among 90 patients, groups 1, 2, and 3 included 30 patients each. The mean age in groups 1, 2, and 3 was 9.4 years, 9.4 years, and 11.0 years, respectively. The surgical success rates one year after surgery for groups 1, 2, and 3 were 80.0%, 73.3%, and 73.3% (chi-square test, p = 0.769), respectively. The undercorrection rates for groups 1, 2, and 3 were 16.7%, 23.3%, and 26.7%, and the overcorrection rates were 3.3%, 3.3%, and 0%, respectively. The mean preoperative near stereoacuities for groups 1, 2, and 3 were 224.3 arcsec, 302.0 arcsec, and 1,107.3 arcsec, and the mean postoperative near stereoacuities were 218.3 arcsec, 214.7 arcsec, and 743.0 arcsec (paired t-test; p = 0.858, p = 0.379, p = 0.083), respectively.
Conclusions
In basic X(T) patients, the amount of angle deviation has no influence on surgical outcomes in unilateral LR recession and MR resection. The near stereoacuities by one year after LR recession and MR resection for intermittent X(T) were not different among patient groups separated by preoperative deviation angle.
Intermittent exotropia, X(T), is the most common type of childhood strabismus in Korea. Various surgical treatments for X(T) have been introduced, including bilateral lateral rectus (LR) muscle recession or unilateral LR muscle recession and medial rectus (MR) muscle resection [1]. Basic X(T) is the most common type of X(T), and the deviation of the angle ranges mainly from 20 to 40 prism diopter (PD) [2].
Basic X(T) is known to progress with a gradual increase in angle of deviation, resulting in worsening stereoacuities [3]. Some studies have reported that the greater the preoperative angle of deviation, the lower the surgical success rate [4]. Several studies have been conducted in patients with a large angle of exodeviation, but they were focused primarily on adults [56789].
A number of studies on the effect of strabismus surgery on stereopsis in patients with X(T) have been reported. Some studies have demonstrated improved distance stereoacuity after intervention [1011]. However, there are controversies surrounding the effect of near stereoacuity in X(T). Some authors have suggested that strabismus surgery improves near stereoacuity, while others reported no change in post-surgery near stereoacuity [1213].
In this study, we evaluated the surgical outcomes of unilateral LR recession and MR resection in patients with basic X(T) in Korea according to their angle of deviation. We also evaluated the effect of strabismus surgery on near stereoacuity in patients with X(T).
Materials and Methods
A retrospective review of medical records was conducted on 592 patients who underwent surgery for basic X(T) between August 2009 and August 2013, under the care of one surgeon. All patients underwent unilateral LR recession and MR resection based on the distant angle of deviation. The minimum required follow-up period after surgery was 12 months. Patients with a history of previous strabismus surgery, amblyopia, paralytic or restrictive strabismus, A or V pattern strabismus, associated vertical deviation or dissociated vertical deviation, ocular disease other than strabismus, or neurologic disorders were excluded. Patients were divided into three groups according to their preoperative angle of deviation: group 1 ≤20 PD, 20 PD< group 2 <40 PD, and group 3 ≥40 PD. Group 3 intrinsically had 30 patients. Thus, 30 age-matched subjects were randomly selected to be in group 1 and group 2. A total of 90 patients were included in the study.
The following patient characteristics were recorded: gender, age at surgery, deviation at distance and near, Worth 4-dot test, constancy of deviation, fixation dominance, presence of lateral incomitance, refractive error, and superior or inferior oblique overaction. Prism and alternate cover testing were performed at 1 / 3 m and 5 m for all patients. Near stereoacuity test was performed by Titmus stereotest (Stereo Optical, Chicago, IL, USA) at 40-cm distance, wearing Polaroid spectacles. Sensory status was also evaluated using the Worth 4-dot test (Gulden Ophthalmics, Elkins Park, PA, USA) at distance (6 m) and near (33 cm) for the degree of sensory fusion. The Worth 4-dot criteria were as follows. Patients who detected four lights were considered to have fusion, those who detected five lights were considered as diplopic, and those who saw two or three lights were considered to be suppressing. Postoperative deviation at distance and near, Worth 4-dot test, and near stereoacuity by Titmus stereotest were measured at one day, one week, three weeks, three months, six months, and 12 months postoperatively.
Unilateral LR recession and MR resection were performed by one surgeon according to Wright's surgical amount [14]. An outcome was considered satisfactory if the distant deviation in the primary position was between ≤10 PD of exophoria/tropia and ≤10 PD esophoria/tropia. Undercorrection was defined as an alignment of >10 PD X(T), and overcorrection was defined as >10 PD of esotropia.
Statistical analyses were performed using IBM SPSS ver. 20.0 (IBM Co., Armonk, NY, USA). One-way ANOVA was used for comparison of preoperative and postoperative characteristics among groups. The chi-square test was used for comparison of near stereoacuities, surgical success rate, undercorrection rate, and overcorrection rate. The paired t-test was used for comparison of preoperative and postoperative stereoacuities. A p-value less than 0.05 was considered statistically significant. For statistical convenience, X(T) was designated as plus (+) and esotropia was designated as minus (-).
Results
Patient characteristics are shown in Table 1. Ninety patients were included, with 43 male (47.8%) and 47 female patients (52.2%). Groups 1, 2, and 3 included 30 patients each. The mean age at surgery was 9.4 years in group 1, 9.4 years in group 2, and 11.0 years in group 3 (one-way ANOVA, p = 0.621) (Table 1). The mean follow-up period was 15.5 ± 4.1 months in group 1, 17.6 ± 5.8 months in group 2, and 18.9 ± 9.2 months in group 3 (one-way ANOVA, p = 0.138) (Table 1).
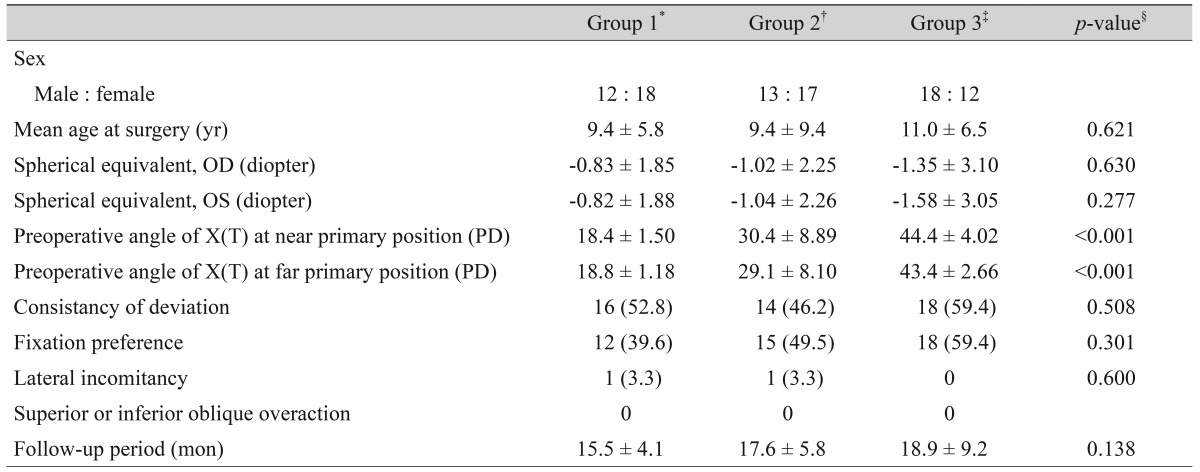
Characteristics of preoperative patients in intermittent exotropia who underwent unilateral lateral rectus recession and medial rectus resection
Postoperative angle of deviation for distant and near fixation of patients with intermittent X(T) in groups 1, 2 and 3 are shown in Table 2. The mean angle of deviation at postoperative one day and one week were significantly different at near and at distance among groups (one-way ANOVA, p < 0.05). However, the mean angles of deviation at later postoperative checks were not statistically different (Table 2).
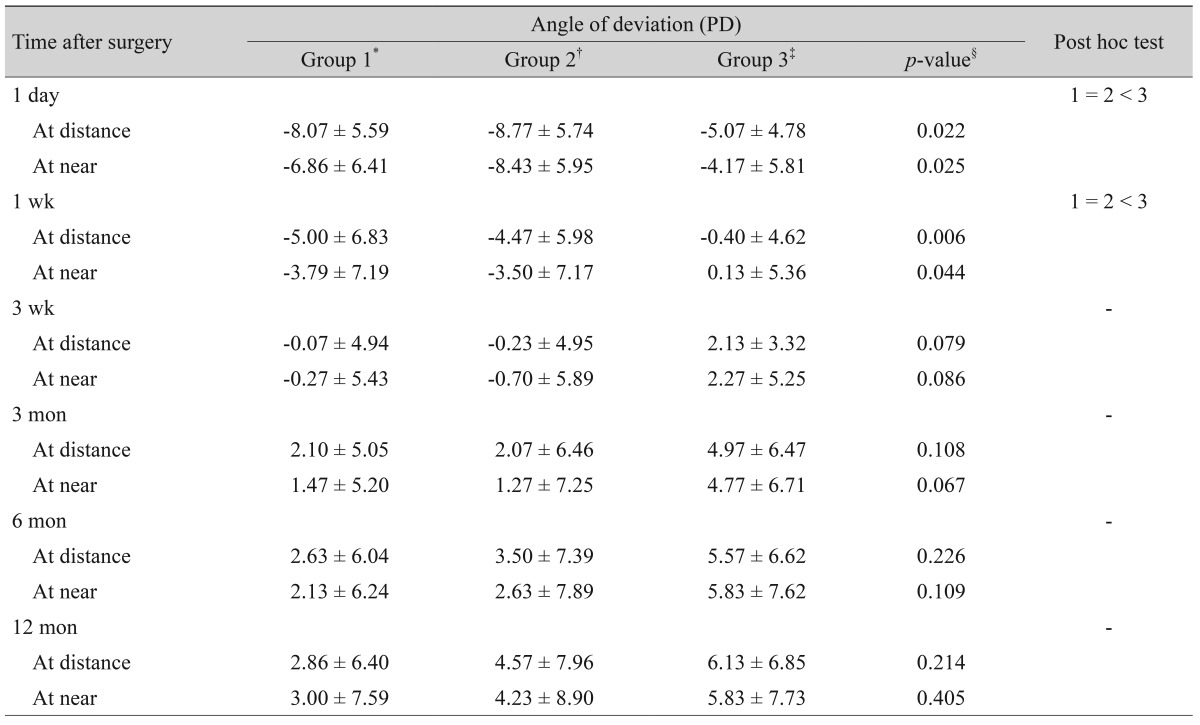
Postoperative angle of deviation for distant and near fixation of patients with intermittent exotropia among groups classified by distance exodeviation
The mean preoperative near stereoacuities were 224.3 arcsec in group 1, 302.0 arcsec in group 2, and 1,107.3 arcsec in group 3. The mean postoperative 12 months near stereoacuities were 218.3 arcsec in group 1, 214.7 arcsec in group 2, and 743.0 arcsec in group 3. In groups 1, 2, and 3, near stereoacuities did not improve postoperatively (paired t-test; p = 0.858, p = 0.379, and p = 0.083, respectively). Among the three groups, group 3 showed significantly different preoperative and postoperative near stereoacuities than the other two groups (one-way ANOVA; p = 0.001 and p = 0.001, respectively). A significantly larger percentage of patients in group 1 and group 2 exhibited superior preoperative near sensory fusional status compared to group 3, as measured using the Worth 4-dot test (chi-square test, p = 0.024) (Table 3). In all groups, near sensory fusion improved postoperatively. In groups 1 and 3, distant sensory fusion improved postoperatively. However, group 2 postoperative distant sensory fusion did not improve.
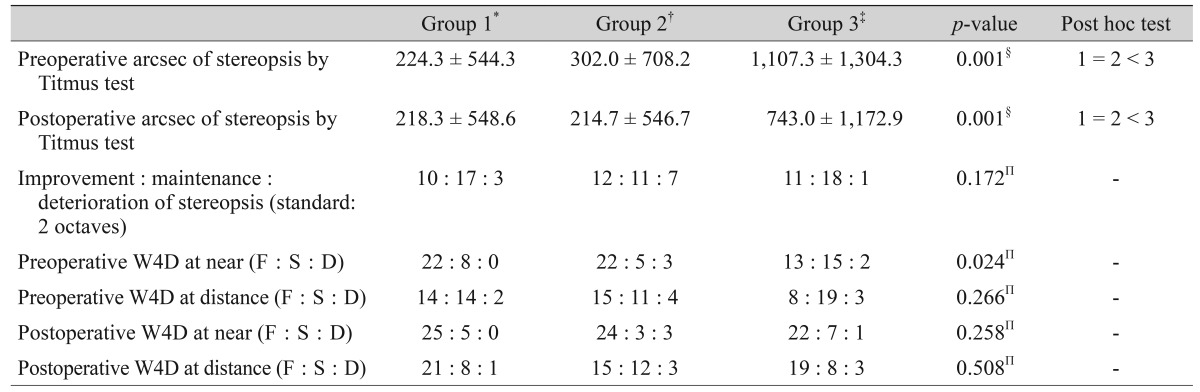
Preoperative and postoperative sensory status of patients with intermittent exotropia among groups classified by distance exodeviation
The rate of surgical success was 80.0% in group 1, 73.3% in group 2, and 73.3% in group 3. Between all three groups, the rates of surgical success were not statistically significant (chi-square test, p = 0.769). In addition, the undercorrection and overcorrection rates were not significantly different among the groups (Table 4).
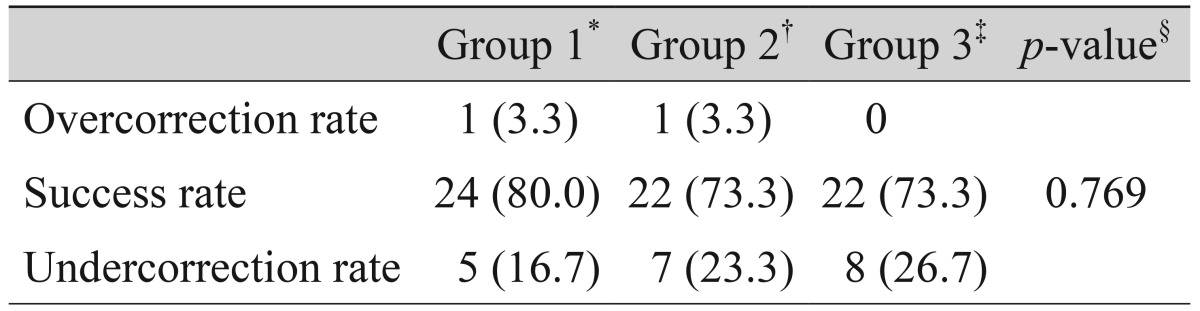
Final surgical outcomes among groups of basic-type intermittent exotropia
Discussion
The surgical success rate of X(T) has been reported to range from 33% to 88% after unilateral LR recession and MR resection procedure [151617]. A number of studies have analyzed the surgical success rates of X(T) with respect to angle deviation, and the surgical success rates have varied from 37.5% to 96.8% [418]. In our study, surgical success rate of the unilateral LR recession and MR resection was 80% in exodeviation under 20 PD, 73.3% in exodeviation between 20 to 40 PD, and 73.3% in exodeviation over 40 PD at one year postoperatively. Currie et al. [8] and Schwartz and Calhoun [9] previously reported that surgical success rates of large angle X(T) were 77%. Additionally, Livir-Rallatos et al. [7] reported that the surgical success rate of exodeviation over 35 PD was 62.0%. Some studies reported that the surgical success rate tended to decrease as the angle of deviation increased [4]. Jeong et al. [18] had reported that the surgical success rate of the unilateral LR recession and MR resection was 67.5% in exodeviation less than 30 PD, 54.0% in exodeviation between 30 to 40 PD, and 37.5% in exodeviation over 40 PD (p = 0.24). In our study, comparably good results were achieved for the unilateral LR recession and MR resection in children with large-angle X(T).
Although a number of studies have been conducted in patients with a large angle of exodeviation, they were focused primarily on adults [56789]. Kim et al. [19] reported that the surgical success rate of unilateral LR recession and MR resection was 68.3% in exodeviation over 40 PD, at more than two-year follow-ups in children. However, they focused on large angle of exodeviation only. In our study, we evaluated the surgical success rate of unilateral LR recession and MR resection in both large angle and moderate angle X(T) in children. To the best of our knowledge, no study comparing surgical outcomes according to angle deviation in X(T) in children has been reported.
Near stereoacuity can be easily measured on an outpatient basis using simple equipment with Titmus stereotest (Stereo Optical) or by TNO stereotest (Lameris Tech., Utrecht, the Netherlands), which is cheap and readily available, and can be performed easily even in children. Baker and Davies [20] reported that 87.1% of X(T) patients' near stereoacuities were not affected by surgical treatment. Simons [21] and Yildirim et al. [22] reported that there were no differences in near stereoacuities of normal eyes and X(T) eyes. In our study, the mean angle of deviation at near stereoacuity at one-year postoperative follow-up was significantly improved. However, near stereoacuities by the Titmus stereotest showed no statistically significant change after surgery. Sharma et al. [11] reported improvement of both distant and near stereoacuity after strabismus surgery in intermittent X(T) patients. Adams et al. [12] reported improvement of distance stereoacuity after surgery, but saw no difference in near stereoacuity outcome. Morrison et al. [13] reported that most cases showed no definite change of stereopsis after surgery in X(T). Our results revealed that realignment at near did not improve near stereoacuities.
Previous studies have proposed that the patients with intermittent X(T) have similar binocular sensory function at near as normal patients until significantly advanced stages [320]. Binocular sensory function at near is stable and surgery cannot be considered as an effective tool for patients with intermittent X(T) [23]. In this study, groups 1 and 2 showed good binocular sensory function at near and were minimally affected by strabismus surgery. However, group 3 showed a relatively deteriorated preoperative binocular sensory function at near which was improved by strabismus surgery. Since group 3 had a larger angle of exodeviation than groups 1 and 2, it could be considered to represent advanced stage of disease. Feng et al. [24] reported that surgical intervention could restore central fusion and stereoacuity in patients with intermittent X(T). Our study showed that binocular sensory function at distance was improved in groups 1 and 3. When defining central fusion as a fusional status both at near and distance, surgical intervention restored central fusion in groups 1 and 3 in our study.
Early postoperative deviation is known to affect the surgical success rate. Keenan and Willshaw [25] reported that early postoperative overcorrection is the only factor that affected postoperative recurrence rate. Scott et al. [26] also reported that early postoperative deviation is important to surgical success rate. Further, Lee and Lee [17] insisted that one day postoperative deviation was a predictive factor in surgical outcome of bilateral LR recession and unilateral LR recession and MR resection. A high surgical success rate has been reported for overcorrection on postoperative day 1 [2728]. In our study, all three groups showed postoperative day 1 overcorrection at distance -8.07 ± 5.59 PD in group 1, -8.77 ± 5.74 PD in group 2, and -5.07 ± 4.78 PD in group 3. All three groups showed postoperative day one overcorrection at near as well. This result might explain the relatively higher surgical success rate in our work.
This study has a few limitations. First, because this was a retrospective study, patients were not randomly assigned to each procedure, which might have caused a selection bias. Second, stereoacuity is variable over time in patients with X(T), which might have affected the validity of our conclusion [2923]. Third, the mean follow-up period is relatively short. Finally, the sample size is small. Therefore, future studies with a larger sample size and longer period of follow-up are highly recommended.
In conclusion, the amount of angle deviation has no influence on surgical outcomes in unilateral LR recession and MR resection in basic X(T) patients. The near stereoacuities after LR recession and MR resection showed no statistically significant differences.
Notes
Conflict of Interest: No potential conflict of interest relevant to this article was reported.