

According to World Health Organization, glaucoma affects more than 13.5 million people over the age of 40, with more than 5 million cases already blind from the disease, as reported by global data in 2002 [1]. It is the second leading cause of blindness worldwide and is expected to affect 80 million people by 2020 [2]. Primary open angle glaucoma (POAG) is more common (1.7%) than primary angle closure glaucoma (PACG, 0.73%). A study conducted by Ramakrishnan et al. [3] found the prevalence of glaucoma in the Indian population to be 2.6%, with 1.7% being POAG, 0.5% being PACG, and 0.3% being secondary glaucoma.
An ideal anti-glaucoma medication would lower the intra ocular pressure (IOP) to the target level without causing any significant systemic adverse events. The pharmacological agents used were miotic medications, adrenergic agonists, b-blockers, carbonic anhydrase inhibitors and newer prostaglandins [4,5]. Like other anti-glaucoma medications, beta-blockers (timolol) and prostaglandins (latanoprost, bimatoprost and travoprost) have been found to be effective in lowering the IOP [6,7].
These drugs have shown variable results in different ethnic populations [5,8,9]. The objective of the present study is to compare the efficacy of latanoprost (0.005%), bimatoprost (0.03%), travoprost (0.004%) and timolol (0.5%) at lowering IOP in patients with POAG, and to determine the incidence of adverse-events of these drugs among the Indian population.
Materials and Methods
Case selection
All the POAG cases that had reported to the Glaucoma Clinic Out-Patient Department of a teaching hospital's tertiary care center between January 2008 and December 2008 and satisfied the inclusion criteria were enrolled. The following inclusion criteria were utilized in this study: newly-diagnosed patients of both genders, age ≥18 years, visual acuity ≥6 / 60 (20 / 200), mean IOP of more than 21 mmHg in one or both eyes, and without any significant difference in diurnal IOP variation, typical glaucomatous optic disc changes with corresponding visual field defects on automated perimetry and wide open angles on gonioscopy. The following patients were excluded from the study: patients on medication for glaucoma, normal or low tension glaucoma, angle closure glaucoma patients with a history of intraocular surgery, diabetes mellitus, hypertension, bronchial asthma, ocular inflammation or infection in the preceding 3 months, conditions precluding Goldmann applanation tonometry, pregnant or lactating women, and patients that are sensitive to preservatives.
Study design
A detailed history, clinical examination and treatment plan were recorded in a standard proforma for each study participant. The Institute Ethics Committee approved the protocol of the study. A written informed consent was collected from each patient at the time of inclusion into the study. One thousand one hundred thirty-two cases were screened for the study; of these, 175 patients satisfied the inclusion criteria and 35 refused to participate. A total of 140 patients were included in the study, and randomized into four groups through computer-generated random table numbers with an equal allocation of 35 patients into each study group. The person enrolling participants into the study knew what medication each study participant had been assigned; thus, the treatment assignments were not concealed from the study enroller. However, the person recording the IOP measurements was unaware of which study medication was assigned to each patient. This same observer recorded measurements prior to the start of the study as well as during the follow-up visits. The following study medications were used (as open label marketed products): group I, patients were given latanoprost (0.005%), once daily; group II, patients were given bimatoprost (0.03%), once daily; group III, patients were given travoprost (0.004%), once daily; group IV, patients were given timolol gel (0.5%), twice daily.
A complete ophthalmic examination including visual acuity, slit lamp examination of the anterior segment, Goldman applanation tonometry, gonioscopy, dilated fundus examination, stereoscopic biomicroscopy for optic cup-disc ratio using a 90-diopter lens, central corneal thickness, IOP variation, and two reliable visual field tests for all patients by Humphrey field analyzer using SITA (Swedish Interactive Thresholding Algorithm) 30-2 program were performed before patients were included in the study.
The four IOP readings (8 a.m., 12 p.m., 4 p.m., and 8 p.m.) were taken in each group a day before each patient was included in the study, and when no significant differences existed among these readings, the patient was enrolled. Baseline IOP values were recorded again on the day of drug allocation. The two IOP measurements were recorded and if the measurement differed by >2 mmHg, a third measurement was also taken. The mean of 2 or 3 readings was recorded as the baseline value. The mean IOP measurements for both eyes was taken and used for analysis in patients who had disease in both eyes and satisfied the inclusion criteria. In patients with bilateral disease who only had one eye that met all the inclusion criteria, data were collected only from the eligible eye. Drugs were self-administered starting the evening of the baseline visit, and one drop of latanoprost (0.005%), bimatoprost (0.03%), or travoprost (0.004%) was applied between 8 to 9 p.m. or one drop of timolol (0.5%) was applied twice daily (between 8 to 9 a.m. and 8 to 9 p.m.) for 3 months. At each study visit, three IOP measurements were taken between 8 to 10 a.m. by one observer who was unaware of which medication had been administered. The mean of these three measurements was used for analysis.
The observations were recorded during four visits: baseline (day 0), week 2, week 6, and week 12. At each visit, the patients were examined for visual acuity (distance and near), evaluation of the anterior segment, fundus evaluation, applanation tonometry, and for ocular and systemic adverse events by a single observer, as per standardized methods. Three readings of each patient's heart rate and blood pressure were measured, and the mean was recorded. The recordings were made on the prestudy day, baseline day when medication regimens were allocated to each study participant, and at every subsequent follow-up visit (Fig. 1).
Statistical analysis
The continuous variables in the treatment group were tested for differences using the one-way ANOVA (analysis of variance test) with treatment (latanoprost, bimatoprost, travoprost or timolol) as the independent variable. If the overall treatment effect was significant (p < 0.05), post-hoc analysis (Bonferroni test) was performed for multiple comparisons between the groups. For paired sample analysis, the Student's t-test was used. The primary effect outcome, as determined by a 95% confidence interval (CI) of the mean difference in IOP values between baseline and week 12, was analyzed using the ANCOVA (analysis of covariance model). The differences in occurrence of side-events were tested using the Fisher exact probability test. The data were analyzed using SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA).
Results
Out of the 140 patients, 19 cases had disease in one eye and 121 cases had disease in both eyes. There were 35 cases in each treatment group, and each group received one of the following medications: latanoprost (0.005%), bimatoprost (0.03%), travoprost (0.004%), or timolol (0.5%). At week 2, one patient was lost to follow-up in the latanoprost, bimatoprost and travoprost groups, and two patients were lost to follow-up in the timolol group. At week 6, three patients were lost to follow-up in the latanoprost group, two in the bimatoprost group, and three in the travoprost group. At the end of the study period (i.e., week 12), three patients had dropped out of the bimatoprost group. The reason why patients did not return for their follow-up visits was not determined. Data from one of the cases in the travoprost group was not included in the data analysis since patient relocated to other city. Thus, data from 124 of the original 140 (88.5%) cases were used in this study (Fig. 1).
Patient characteristics in the different study groups are presented in Table 1. The mean age, proportion of males and females, cup-disc ratio, and central corneal thickness were comparable in all four study groups. Family history of glaucoma was found in 14.3% of the patients in the latanoprost and bimatoprost groups, 20% in the travoprost group, and 17.1% in the timolol group. The IOP measurements were recorded at 8 a.m., 12 p.m., 4 p.m., and 8 p.m. for each patient. The mean IOP values did not differ significantly among the different groups at each individual time point, nor were the overall IOP values different.
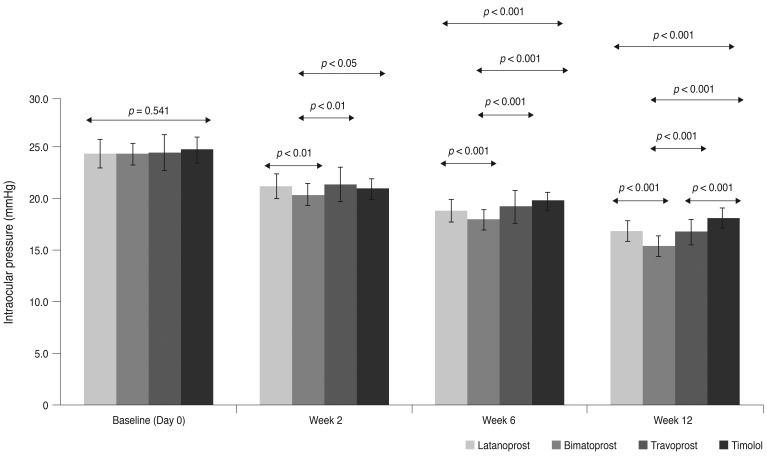
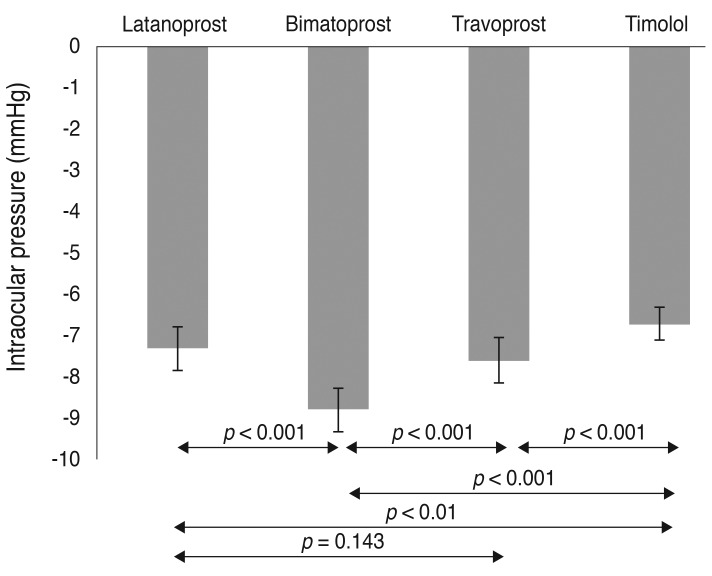
The mean IOP values in the different study groups that were recorded at baseline (day 0), week 2, week 6, and week 12 are shown in Fig. 2. The following mean IOP levels were recorded at baseline: 24.5 mmHg in the latanoprost and bimatoprost groups, 24.6 mmHg in the travoprost group, and 24.9 mmHg in the timolol group (p = 0.541). There was a significant reduction in values from baseline at each of the time points (p < 0.001), and the amount of reduction was different among groups at week 2 (p < 0.01), week 6 (p < 0.001), and week 12 (p < 0.001). The mean reduction in IOP (mmHg) at week 12 compared to baseline (p < 0.001) was significantly greater in the bimatoprost group (8.8 ± 1.1) compared to the latanoprost group (7.3 ± 1.1), travoprost group (7.6 ± 1.0), and timolol group (6.7 ± 0.8). Latanoprost and travoprost were comparable in efficacy (p = 0.143) (Fig. 3). The mean IOP reductions were significantly different among the groups; specifically, the bimatoprost group (-2.71; 95% CI, -2.25 to -3.18), travoprost group (-1.27; 95% CI, -0.81 to -1.27), and latanoprost group (-1.25; 95% CI, -0.79 to -1.71) in comparison to the timolol group at week 12 (p < 0.001). The bimatoprost group had a significantly higher reduction in IOP when compared to the travoprost and latanoprost groups (p < 0.001).
Among the different drugs studied, bimatoprost (35.9 ± 3.5) caused a significantly higher mean percent reduction in IOP at week 12 than latanoprost (29.9 ± 3.5), travoprost (30.8 ± 2.6) and timolol (26.6 ± 2.3), when compared to baseline values (p < 0.001). Latanoprost and travoprost did not show any significant difference in mean IOP reduction (p = 0.126) (Fig. 4).
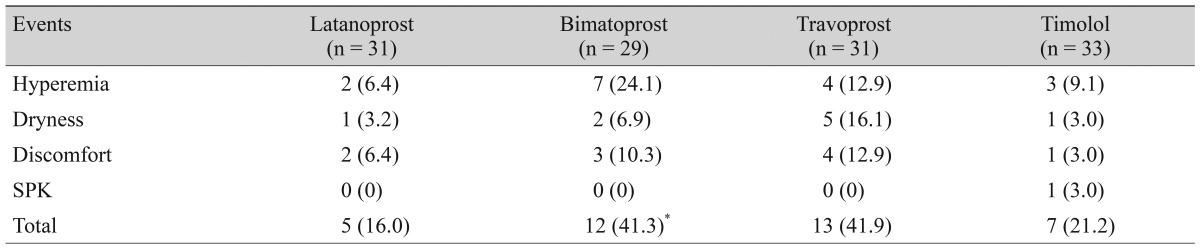
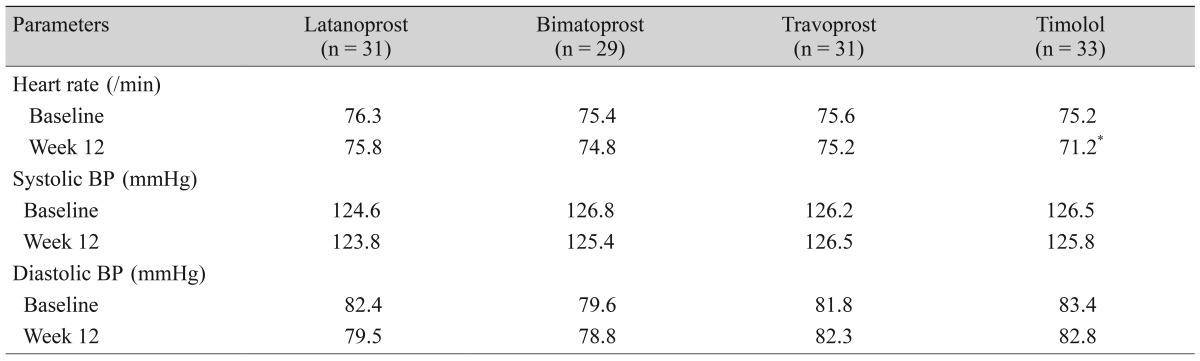
The adverse events observed over the study period for each drug are presented in Table 2. The most significant adverse events were found in about an equal proportion of patients treated with each drug-bimatoprost (41.3%) and travoprost (41.9%) followed by timolol (21.1%) and latanoprost (16.0%). The bimatoprost group had a significantly higher percentage of adverse events compared to the latanoprost group (p < 0.05). Patients complained of conjunctival hyperemia with bimatoprost (24.1%), and dryness of the mouth with travoprost (16.1%). Superficial punctuate keratitis and cough were seen only in the timolol group. In addition, only patients in the timolol group showed a significant decrease in mean heart rate (per minute) at week 12 in comparison to baseline values (p < 0.001). The mean systolic and diastolic blood pressures recorded in the latanoprost, bimatoprost, travoprost and timolol groups did not differ significantly at week 12 when compared to their baseline values (Table 3).
Discussion
POAG is a chronic and often symmetrical disease where acquired loss of optic nerve fibers and abnormalities in the visual field occur with an open normal appearing angle, and develops insidiously without any outward warning signs. This disease ultimately progresses to optic nerve atrophy. Early detection and reduction of IOP prevents the disease from further progression.
Timolol (0.5%) showed a significant reduction in mean IOP (-6.7 mmHg, 26.6%) from baseline in our patients at the end of week 12. In a meta-analysis of randomized controlled trials, Zhang et al. [10] reported the IOP lowering effect of timolol to be 26.9% at the 3 months follow-up visit. In the latanoprost (0.005%) group, the reduction of IOP at the end of the study was 29.9%. Similar reductions (29% to 31%) were shown by Parrish et al. [7] and Gandolfi et al. [11], whereas Noecker et al. [12] found a lower IOP reduction (24.1%) as compared to our study.
The mean IOP reduction seen with bimatoprost administration from baseline were significant at all three visits with the maximum reduction (35.9 %) occurring at week 12. A similar reduction (35.1%) was observed by Tuna et al. [13]. The maximum IOP reduction of 30.9% with travoprost administration was observed at week 12. Yildirim et al. [14] and Goldberg et al. [15] also observed a similar range (30% to 31%) of IOP reductions in their patients.
An attempt was also made to determine the comparative efficacy of prostaglandin analogues with timolol, and it was observed that bimatoprost showed better efficacy than the other prostaglandins. Stewart et al. [5] also reported a greater IOP reduction with prostaglandin analogues when compared to timolol.
Among prostaglandin analogues, Parrish et al. [7] reported equal efficacy of these drugs. However, in our study, bimatoprost showed a significantly greater mean IOP reduction (p < 0.001) in comparison to latanoprost and travoprost; the latter two had comparable efficacy. Aptel et al. [16] reported similar findings in a systematic meta-analysis of trials. In contrast, the amount of IOP reduction seen at 8 and 10 a.m. in the travoprost group (31%) was significantly higher (p < 0.001) when compared to patients treated with latanoprost (19.7%) and bimatoprost (21.6%), as reported by Yildirim et al. [14] during an 8-week trial period. However, we found that bimatoprost showed greater efficacy in IOP reduction compared to the other drugs at every follow-up visit. This difference in drug response might be due to variations in drug effects in different populations.
All of the four study drugs produced significant reductions in IOP individually. However, it is difficult to commcomment on the statistically-significant differences in IOP reductions among the drugs with respect to clinical relevance since it was not feasible to determine suitable outcome data for such a purpose in this study.
The intraocular pressure control depends on aqueous flow, which follows the circadian rhythm, with a lower flow rate at night. Thus, a drug like timolol, which lowers IOP by reducing aqueous formation, is less effective at night. Prostaglandin analogues lower IOP by enhancing aqueous outflow through the uveo-scleral pathway; this has been shown to be effective both during the day and night. In the present study, latanoprost, bimatoprost and travoprost showed better efficacy in reducing IOP even 12 hours after the nighttime dose administration, when compared to timolol; and the effect was shown to be maximal at the end of week 12. Bimatoprost lowers IOP by increasing aqueous outflow through a pressure sensitive mechanism as well as a pressure insensitive mechanism [4]. This indicates that bimatoprost possibly has a better IOP lowering effect than latanoprost and travoprost.
The safety profile of the study medications was also analyzed, and only the most significant events were recorded for each drug. The studies conducted by Zhang et al. [10] and Brandt et al. [17] observed significant decreases in heart rate with timolol administration, and this could be due to the b-blocker effect of the drug due to its systemic absorption. Though there was a significant decrease in heart rate with timolol administration at week 12 compared to the baseline measurements, this decrease may not be clinically significant because there was no reduction in blood pressure and no symptomatic changes.
Overall, patients treated with bimatoprost had a significantly higher percentage of total adverse-events when compared to patients treated with latanoprost (p<0.05). Conjunctival hyperemia was seen most frequently with bimatoprost (24.3%) when compared to the other study medications. Honrubia et al. [18] also reported a similar finding in their meta-analysis of randomized controlled clinical trials. Furthermore, DuBiner et al. [19] also reported other events such as dryness of the eye and discomfort, with bimatoprost use. Superficial punctate keratitis was seen in one patient with timolol administration; this was treated and resolved. The study patients tolerated medications well as was evident during the follow-up visits. The exact reason for loss to follow-up of some patients could not be ascertained. In conclusion, the prostaglandin analogues, latanoprost, bimatoprost and travoprost, had a better IOP lowering effect in patients with primary open angle glaucoma than timolol. Bimatoprost showed the best efficacy out of the prostaglandins studied. The findings from this present study could be very useful to treat IOP in the Indian population.
This study encountered the following limitations: this was an open label trial study, the follow-up periods were relatively short (12-week period), and the sample size in each group was small. A study with adequate allocation concealment and a larger sample size and longer observation period should be undertaken to confirm the comparative therapeutic efficacy of these study medications.



 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






