Bone Marrow-derived Mesenchymal Stem Cells Affect Immunologic Profiling of Interleukin-17-secreting Cells in a Chemical Burn Mouse Model
Article information
Abstract
Purpose
This study investigated interleukin (IL)-17-secreting cell involvement in sterile inflammation, and evaluated the effect of mesenchymal stem cells (MSCs) on IL-17-secreting cell immunologic profiling.
Methods
Twenty mice were sacrificed at time points of 6 hours, 1 day, 1 week, and 3 weeks (each group, n = 5) after the cornea was chemically injured with 0.5N NaOH; IL-17 changes in the cornea were evaluated using enzyme-linked immunosorbent assay. Further, IL-17 secreting cells were assessed in the cervical lymph nodes by a flow cytometer. Rat MSCs were applied intraperitoneally in a burn model (n = 10), IL-17-secreting T helper 17 (Th17) cell and non-Th17 cell changes were checked using a flow cytometer in both cornea and cervical lymph nodes at 1week, and compared with those in the positive control (n = 10).
Results
IL-17 was highest in the cornea at 1 week, while, in the cervical lymph nodes, IL-17-secreting cells showed early increase at 6 hours, and maintained the increase through 1 day to 1 week, and levels returned to the basal level at 3 weeks. Specifically, the non-Th17 cells secreted IL-17 earlier than the Th17 cells. When the MSCs were applied, IL-17 secretion was reduced in CD3(+)CD4(-)CD8(-), CD3(+)CD4(+)CD8(-), and CD3(+) CD4(-)CD8(+) cells of the cervical lymph nodes by 53.7%, 43.8%, and 50.8%, respectively. However, in the cornea, IL-17 secretion of CD3(+)CD4(-)CD8(-) cells was completely blocked.
Conclusions
The results indicated that both IL-17-secreting non-Th17 and Th17 cells were involved in the chemical burn model, and MSCs appeared to mainly modulate non-Th17 cells and also partially suppress the Th17 cells.
Mesenchymal stem cells (MSCs) are reported to have self-renewal capacity for multipotent differentiation, and immunomodulatory properties. MSCs have been studied for therapeutic purposes in various fields. MSCs have been known to modulate both innate and adaptive immunity, through the suppression of T cells, B cells, dendritic cells, natural killer (NK) cells, macrophages and neutrophils, and they have been investigated as therapeutic targets because of their ability to intervene in autoimmune disease or inflammatory disease [1,2,3,4].
The T helper 17 (Th17) cell was extensively investigated as a critical factors that can cause various autoimmune diseases or inflammatory diseases [5,6,7,8]. In addition, recent studies highlighted the function of innate and adaptive interleukin (IL)-17-secreting cells with variable cell sources in various inflammatory diseases [9]. The IL-17 receptor is ubiquitously expressed throughout the body, resulting in pleiotropic actions of IL-17 on a wide range of cell types. One of the well-known biological outcomes of IL-17 signaling is the induction of proinflammatory cytokines and chemokines from target cells, such as fibroblasts and epithelial cells, leading to the recruitment of neutrophils [10]. The primary function of activated neutrophils is to fight against invading pathogens, but this can damage the surrounding tissues. There have been numerous research studies to determine the immune-modulatory role of MSCs on the Th17 cells [11,12,13,14,15], however, only a few studies had investigated the effect of MSCs on other sources of IL-17-secreting cells, including innate lymphoid cells or gammadelta T-cells [16].
The MSC-based cellular therapy could be applied to treat graft versus host disease and autoimmune disease. In addition, MSCs have been exploited for many ocular disease treatments, such as corneal disease, uveitis and retinal diseases. In functional disabilities, such as ocular blindness, chemical burns often occur as an occupational hazard and can induce severe inflammation through both innate and adaptive immunity, including IL-17-secreting cells [17]. In fact, the anti-inflammatory effect of MSCs has recently been studied in chemically injured eyes [18,19,20,21,22]. However, the function of the innate and adaptive IL-17-secreting cells in inflammation has not yet been determined in a chemical burn model, and the effects of MSCs on the innate and adaptive IL-17-secreting cells have not been investigated in this model either.
Therefore, we hypothesized that both innate and adaptive IL-17-secreting cells may be involved in the inflammation that results after chemical injury to the cornea. First, we investigated time-dependent immunologic profiling of both innate and adaptive IL-17-secreting cells in a chemically-injured animal model, and then we determined the effect of bone-marrow derived MSCs on both innate and adaptive IL-17-secreting cells in this model.
Materials and Methods
Animals
Five-week-old male C57BL/6 mice, weighing 30 g, were purchased from the Orient Bio (Seongnam, Korea). All animal experiments were conducted in accordance with the ARVO Statement for the Use of Animals in Ophthalmic and Vision Research. The experimental protocols were approved by the Institutional Animal Care and Use Committee of the Seoul National University Hospital (permit number 11-0212).
Corneal chemical burn model and time-dependent changes of interleukin-17 in the model
Mice were anesthetized with an intraperitoneal injection of zolazepam (Zoletil; Virbac Laboratories, Carros, France; 0.006 mL/10 g) and xylazine hydrochloride (Rompun; Bayer, Frankfurt, Germany; 0.004 mL/10 g). To create the chemical injury, a 6-mm filter paper soaked in 100% ethanol was applied to the whole cornea of the left eye, including the limbus for 30 seconds, followed by a rinse with 10-mL of balanced salt solution, then the corneal and limbal epithelium were removed with a surgical blade. Next, a 6-mm filter paper soaked in 0.5N NaOH was applied to the corneal surface for 15 seconds, followed by rinsing with 20-mL of balanced salt solution. Ofloxacin ophthalmic ointment was instilled immediately.
To investigate the changes of IL-17, twenty mice, which had undergone the cornea chemical burn procedure, were sacrificed at times point of 6 hours (n = 5), 1 day (n = 5), 1 week (n = 5), and 3 weeks (n = 5) after injury. To evaluate the inflammatory cytokines changes in the cornea, all injured corneas were harvested and were pooled to evaluate cytokine changes in enzyme-linked immunosorbent assay (ELISA). The cervical lymph nodes were evaluated to assess IL-17-secreting cell changes using a fluorescent-activated cell sorter (FACS) analysis at each time point.
Mesenchymal stem cells preparation and application
Rat primary MSC lines (cryopreserved rat mesenchymal stem cells, part no. 2004005; Millipore, Temecula, CA, USA) were thawed, according to the manufacturer's instructions. The cells were resuspended and cultured in alpha minimum essential medium (Invitrogen-GIBCO, Carlsbad, CA, USA), supplemented with 10% fetal bovine serum (Atlanta Biological, Lawrenceville, GA, USA), Penicillin/Streptomycin (100 U/mL, Invitrogen-GIBCO) and 200 mM L-glutamine (Invitrogen-GIBCO) for 72 hours in a T75 flask. The cells were plated in a flask at a density of 1 × 106 cells/cm2 and incubated at 37℃ with 5% CO2. The media was exchanged every two days, and after 10 to 14 days, the non-adherent cells and supernatant were discarded. Adherent cells were treated with Accutase (Millipore) for three minutes and replated in a new flask at 5 × 103 cells/cm2. Adherent cells, obtained after the second subculture, were used for the experiment.
Thirty mice were randomly divided into three groups (each group, n = 10). The first group was the positive control group that received chemical injury to the cornea by the method mentioned above and the negative control group did not receive chemical injury. The second group was the treatment group, and the mice were given intraperitoneal injections of the media, including rat MSCs (5 × 106/200 µL) after the chemical injury. All the mice were sacrificed at 1 week after injury.
Cytokine quantification by enzyme-linked immunosorbent assay
To investigate the time-dependent change of inflammatory cytokines in the cornea based on the chemical burn model, the corneal samples at different time points after injury were lysed in protein extraction buffer (PRO-PREPTM Solution; Intron Biotechnology, Seongnam, Korea), and were centrifuged at 2,500 rpm for 20 minutes. An aliquot of each supernatant was assayed. The concentrations of cytokines were measured using an ELISA, according to the manufacturer's recommendations (R&D systems, Minneapolis, MN, USA) at 450 nm that included IL-6, IL-17, tumor necrosis factor alpha (TNF-α) and interferon gamma (IFN-γ). The analysis was performed with the pooling of the cornea at each time point with duplicates.
Fluorescent-activated cell sorter analysis for interleukin-17-secreting cells in the cornea and cervical lymph nodes
To assess the changes of IL-17-secreting cells in the cornea and the cervical lymph nodes between the positive control group and the treatment group, the mice was sacrificed at 1 week. The left cornea of each mouse was pooled in each group and was excised from the eyeballs, sliced with scissors into small pieces, and the tissue was homogenized with a sonicator (Tomy-Seiko, Tokyo, Japan). The samples were incubated at 37℃ for 1 or 2 hours (2 mg/mL collagenase D [Roche Diagnostics, Indianapolis, IN, USA] with 0.05 mg/mL DNase [Roche]) and were centrifuged at 1,200 rpm for 10 minutes. An aliquot of each supernatant was passed through a 70-µm cell strainer (BD Falcon, San Jose, CA, USA) for single cell suspension. The cells were counted, using trypan blue dye and an automated cell counter (Countess; Invitrogen, Carlsbad, CA, USA), and were prepared for IL-17-secreting cell staining.
Left cervical lymph nodes from each mouse were extracted and were pooled in each group. The lymph node cells were isolated and resuspended in the DMEM media, including 1% HEPES and 0.5% FBS for FACS analysis. Lymphocytes were stimulated with 50 ng/mL phorbol myristate acetate (Sigma-Aldrich, St Louis, MO, USA), 1 µg/mL Ionomycine (Sigma Aldrich) and 1 µg/mL GolgiPlug (BD Phamingen, San Diego, CA, USA) for 5 hours. The cells were then rinsed twice with FACS buffer (0.002% sodium azide, 0.2% BSA/PBS; eBioscience, San Diego, CA, USA) and resuspended in fixation solution (BD Phamingen) for intracellular cytokine staining. The protocol was performed based on the manufacturer's instructions.
The cells isolated from the left cervical lymph node and left cornea were stained with fluorophore-conjugated antibodies: PerCP-conjugated anti-CD3 (eBioscience), FITC-conjugated anti-CD4 (eBioscience), PE-cy7-conjugated anti-CD8 (eBioscience), APC-conjugated anti-IFNγ (eBioscience), or PE-conjugated anti-IL-17 (BD Phamingen). Absolute cell numbers were calculated by multiplying the percentage of positive staining cells in the total acquired events by the total number of cells isolated from the analyzed tissue. Immunofluorescence was analyzed with Flowjo software ver. 7.6.5 (Treestar, Ashland, OR, USA) with a FACS Caliber flow cytometer (FACS Canto; Becton Dickinson, San Diego, CA, USA).
In the MSCs applied group, the decrease of the IL-17-secreting cells was presented as the reduction rate. The reduction rate was calculated with the following formula: (pretreatment - posttreatment) × 100 / pretreatment.
Statistical analysis
The cervical lymph nodes were examined to assess changes in the IL-17-secreting cells. The lymph nodes were assessed with FACS analysis at each time point and were compared with the positive control group by a Moses test of extreme reactions using SPSS ver.17.0 (SPSS Inc., Chicago, IL, USA). For statistical analyses, a p-value of <0.05 was considered statistically significant.
Results
Time-dependent changes in inflammatory cytokines after chemical injury in the cornea
First, we used ELISA to look at the cytokine changes in the cornea. The analysis showed that the production of IL-17 cytokines was the highest (46.95 pg/mL) at 1 week, and returned to almost the basal level (0.944 pg/mL) at 3 weeks after injury. Similarly, TNF-α levels increased at 1 week and then decreased at 3 weeks. In contrast, IL-6 showed the highest peak at 6 hours, and was subsequently reduced over time. However, IFN-γ was not detected throughout the entire post-injury time period (Fig. 1). We hypothesize that the IL-17-secreting cells maximally infiltrated into the cornea 1 week after the injury.
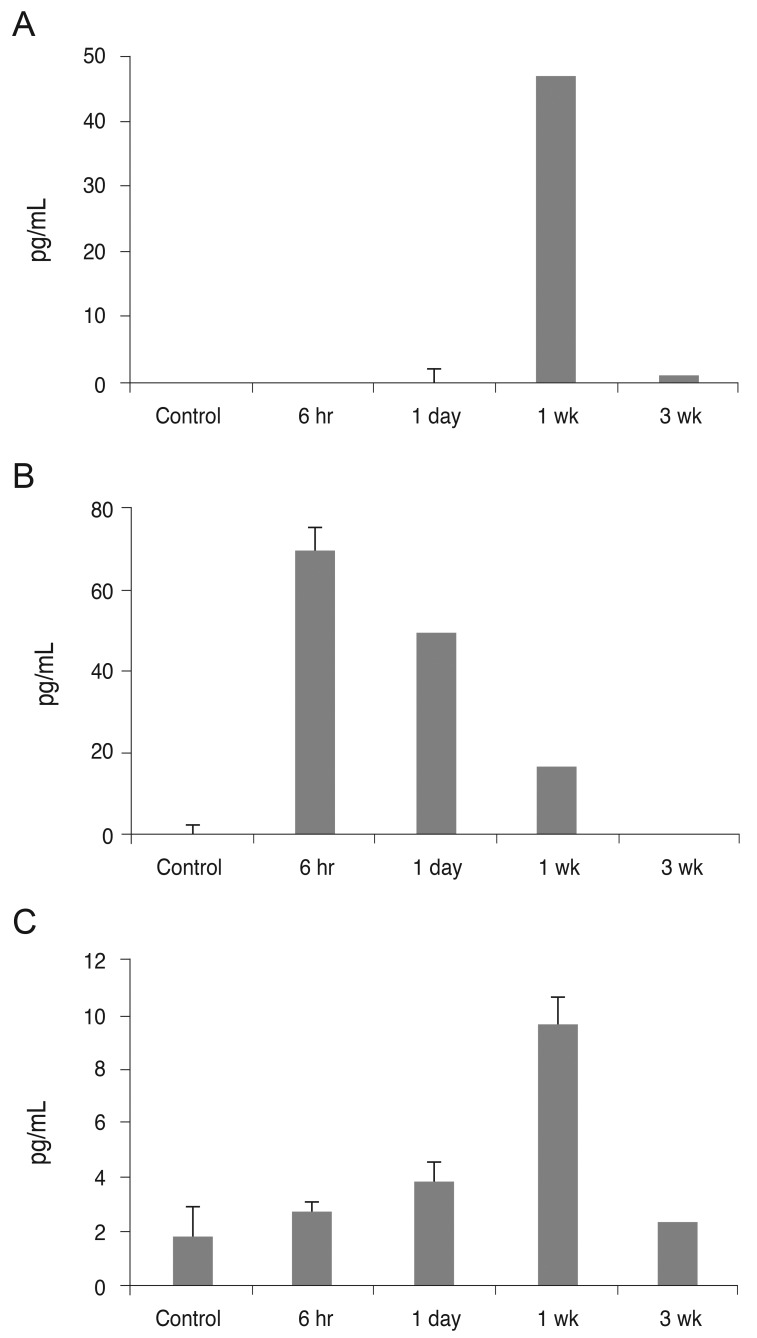
Enzyme-linked immunosorbent assay analysis of the corneal lysate after chemical injury. The bar charts show the mean concentrations of pro-inflammatory cytokines. (A) Interleukin (IL)-17. (B) IL-6. (C) Tumor necrosis factor alpha (TNF-α). Control represents the normal cornea. Note that the production of cytokines IL-17 and TNF-α peaked at 1 week post-injury, and in contrast, peak IL-6 levels increased immediately after injury. The experiments were performed in duplicate.
Time-dependent immunologic profiling of interferon gamma and interleukin-17-secreting cells in chemical injury
Next, we examined systemic changes of IFN-γ and IL-17-secreting cells in the chemically-injured mouse model. We analyzed changes in sub-population secretion of IFN-γ and IL-17 in the cervical lymph nodes, based on the following outline (Fig. 2); CD3(-)CD4(-) cells, which included innate lymphoid cells and B cells; CD3(+)CD4(-) cells, which included gammadelta T-cells, NK cells, NK T-cells or CD8(+) T-cells; and CD3(+)CD4(+) cells, which represented CD4 T helper cells.
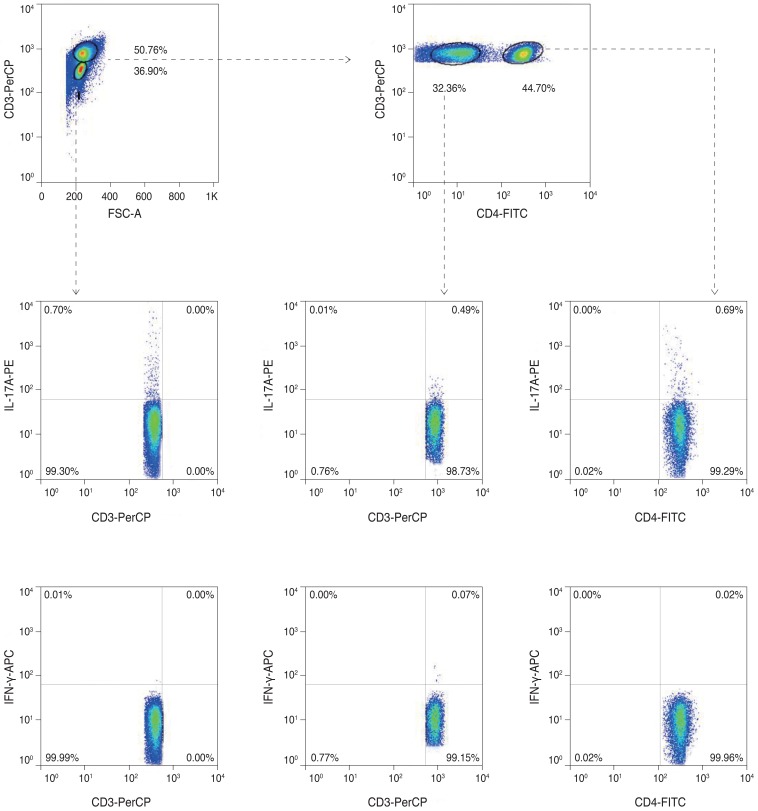
This photo represented a sort-out analyses of the interleukin (IL)-17/interferon gamma (IFN-γ) secreting cells in the cervical lymph nodes, following corneal chemical injury. The non-Th-cells (CD3(-)CD4(-) cells or CD3(+)CD4(-) cells) and CD3(+)CD4(+) T helper cells were separated and were analyzed.
The results indicated that of the IFN-γ secreting cells, only CD3(+)CD4(-) cells showed high increases of IFN-γ at day 1 after the procedure, and the numbers abruptly decreased from 1 to 3 week measurements (Fig. 3). A thorough analysis of the CD3(-)CD4(-) cells and the CD3(+)CD4(-) cells at day 1, and the CD3(-)CD4(-) cells at 3 weeks indicated that the cells numbers were significantly greater than the negative control group. This result suggests that the non-Th17 cells (gammadelta T-cells, NK cells, NK T-cells, and CD8(+) T-cells) were temporarily activated.

The bar charts show the mean (A) percentages and (B) cell numbers of the interferon gamma (IFN-γ) secreting cells in the cervical lymph nodes of the 4 groups (each group, n = 5), divided over the time course of 6 hours, 1 day, 1 week, and 3 weeks after the onset of chemical injury. Note that IFN-γ-secreting non-Th-cells (CD3(-)CD4(-) T-cells) reached the highest peak at day 1 after injury, and the Th-cells also increased at 1 day before the levels returned to baseline. *p < 0.05 (Moses extreem reactions test).
In comparison, the IL-17-secreting cells showed an early increase at 6 hours, and the elevated level of IL-17 was maintained through day 1 to 1week and returned to the basal level at 3 weeks (Fig. 4). A thorough analysis of the CD3(-)CD4(-) cells at day 1 and the 1 to 3 week time interval indicated that the CD3(+)CD4(+) cells at 6 to 24 hours, and the CD3(+)CD4(-) cells at 6 to 24 hours and 1 week had significantly increased numbers when compared with the negative control group. Specifically, the non-Th17 cells (CD3(-)CD4(-) cells and CD3(+)CD4(-) cells) secreted IL-17 earlier than CD3(+)CD4(+) Th17 cells; CD3(+)CD4(+) Th17 cells secreted IL-17 over 1 day.
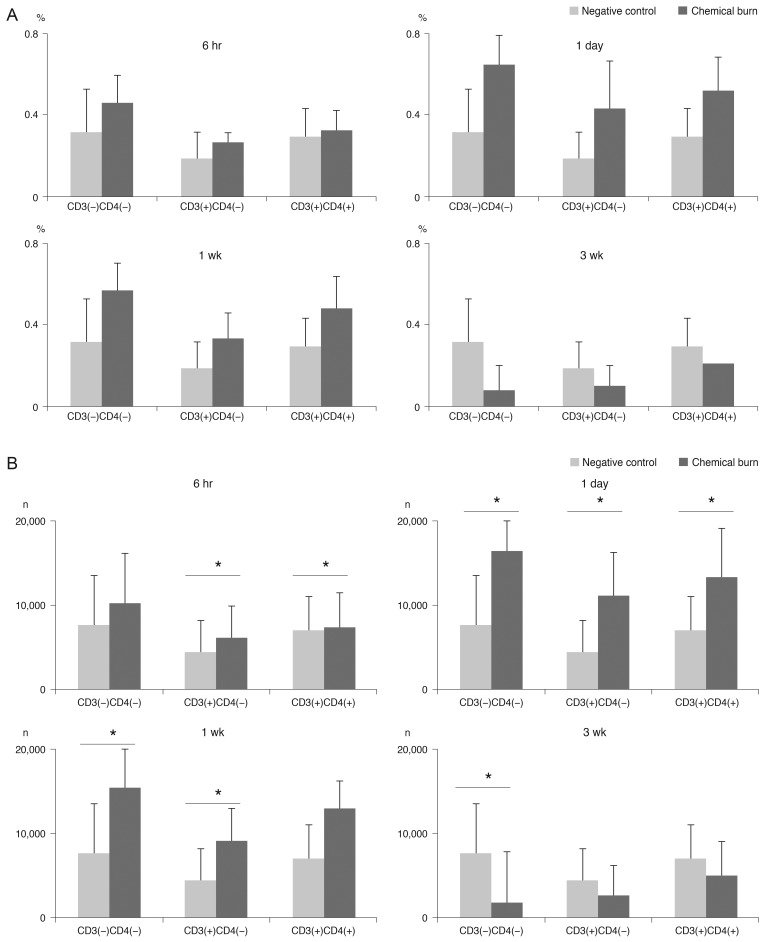
The bar charts show the mean (A) percentages and (B) cell numbers of the interleukin-17-secreting cells in the cervical lymph nodes in the 4 groups (each group, n = 5), divided over the time course of 6 hours, 1 day, 1 week, and 3 weeks after the onset of chemical injury. Note that both the non-T helper 17 (Th17) cells and Th17 cells increased 1 week after injury, and then gradually decreased. *p < 0.05 (Moses extreem reactions test).
Mesenchymal stem cells effect on interleukin-17-secreting cells in a chemical burn model
Although IL-17-secreting cells were systemically elevated from 6 hours to 1 week, the cornea showed the highest peak level of IL-17 at 1 week. Therefore, we chose the time point of 1 week to assess the anti-inflammatory effect of MSCs on the IL-17-secreting cells. The IL-17 secretion was reduced by 53.7%, 43.8%, and 50.8% in CD3(+)CD4(-)CD8(-) cells, CD3(+)CD4(+)CD8(-) cells (Th17), and CD3(+)CD4(-)CD8(+) cells, respectively, of the cervical lymph nodes when MSCs were applied (Fig. 5). Additionally, analysis of the cornea indicated that IL-17 secretion from CD3(+)CD4(-)CD8(-) cells was completely blocked, while the secretion of IL-17 in the CD3(+)CD4(+)CD8(-) cells (Th17 cells) was partially reduced by 10.5% (Fig. 6). IL-17-secreting CD3(+)CD4(-)CD8(+) T-cells were not detected in the cornea. This result suggested that MSCs mainly modulate CD3(+)CD4(-)CD8(-) non-Th17 cells, and also partially suppress CD3(+)CD4(+)CD8(-) Th17 cells to inhibit IL-17 secretion in a chemical burn model.
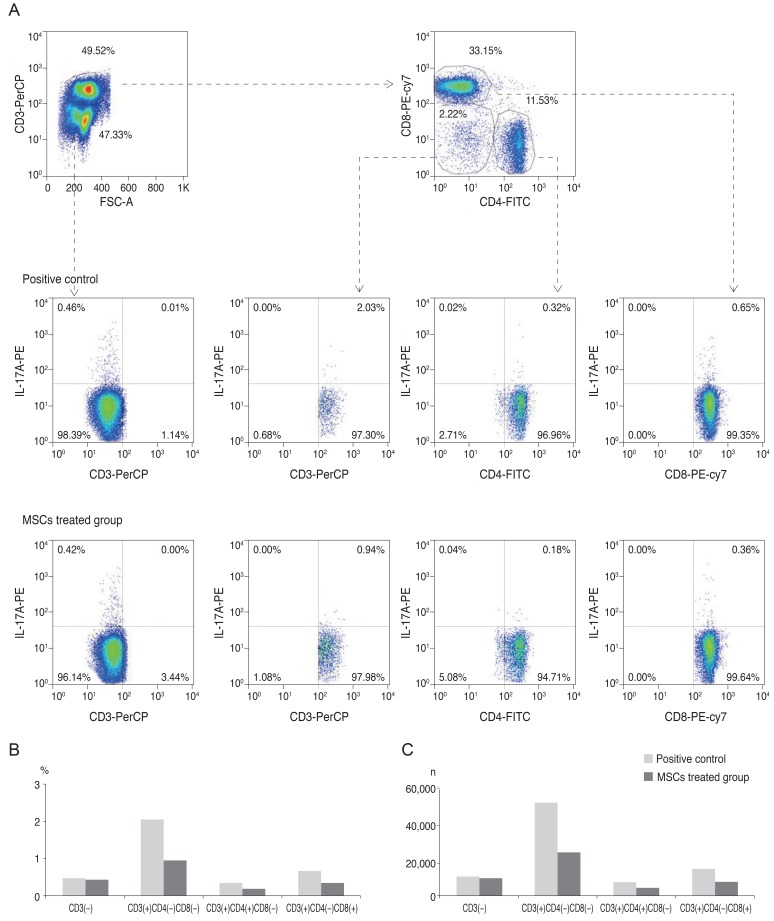
Fluorescent-activated cell sorter analysis of cervical lymph nodes on day 7 (A), following corneal chemical injury in the group treated with mesenchymal stem cells (MSCs) and the control group (each group, n = 10). The bar charts show the (B) percentages and (C) cell numbers of interleukin (IL)-17=secreting cells in cervical lymph nodes. Both non-T helper 17 (Th17) cells (CD3(+)CD4(-)CD8(-) and CD3(+)CD4(-)CD8(+)) and Th17 cells were effectively reduced in the group treated with MSCs. All of the cervical lymph nodes for each group were pooled to perform the experiment.

Fluorescent-activated cell sorter analysis of corneas on day 7, following corneal chemical injury in the group treated with mesenchymal stem cells (MSCs) and the control group. The bar charts show the (A) percentages and (B) cell numbers of the interleukin (IL)-17-secreting cells in the corneas. Complete blockage of IL-17-secreting and the non-T helper 17 cells (CD3(+)/CD4(-)/CD8(-) cells) was shown in the MSC treated group. All of the cornea and lymph nodes for each group were pooled to perform the experiment.
Discussion
Our study revealed that both innate and adaptive IL-17-secreting cells were involved in chemically injured eye recovery, and that MSCs effectively suppressed IL-17 secretion in this model by blocking both CD3(+)CD4(-)CD8(-) non-Th17 cells and CD3(+)CD4(+)CD8(-) Th17 cells. To our knowledge, this is the first report to determine which cells are modulated by MSCs to attenuate IL-17 secretion in an ocular chemical burn model.
Systemically, in response to burn injury, IL-1β, TNF-α, and IL-6 are initially increased. However, after an initial pro-inflammatory phase, studies have determined that burn injury can result in a loss of Th1 cells, associated with depressed levels of IFN-γ and a concomitant increase of Th2 cells. In regards to innate immunity, decreased macrophages and NK cells have been reported to increase the susceptibility of infection [23].
The initial responses of neutrophils and macrophages were time-dependent and the analysis in ocular chemical burn conditions was well dissected in order to understand innate immune reactions [24]. T cell involvement in ocular burns, as an adaptive immune response, was also reported, including the Th17 cells [17,25,26]; however, the details of T cell involvement have not been determined in sterile inflammation.
Our chemical burn model showed that IL-17 was involved in the sterile inflammation process. ELISA data revealed high IL-17 levels in the cornea at 1 week. However, contrary to IL-6, which was increased after 6 hours, the response of IL-17 appeared delayed; therefore we questioned the main sources of IL-17. There are numerous sources that discuss IL-17-secreting cells, and the major cell sources of IL-17A and IL-17F are known to be Th17 cells, gammadelta T-cells, innate lymphoid cells, NK cells, NK T-cells, and CD8(+) T-cells. In addition, gammadelta T-cells are crucial players in the barrier function of mucosal immunity and with the skin, including the eyes. Our results implied that non-Th17 cells (gammadelta T-cells, NK cells, NK T-cells, or CD8(+) T-cells) in addition Th17 cells seemed to be involved in the secretion of IL-17 in the early stage of the chemical burn model. The suppression effect of MSCs was more prominent on the non-Th17 cells (gammadelta T-cells, NK cells, and NK T-cells), which secreted IL-17, instead of on the Th17 cells in the cornea. This result provides indirect in vivo evidence in addition to recent in vitro recent evidence that MSCs can inhibit gammadelta T-cells and NK T-cells [16]. Although MSCs inhibit Th17 cells [11,12,13,14,27], MSCs seem to modulate the IL-17-secreting cells, Th17 cells, and also non-Th17 cells in sterile inflammation.
Although the results in this study cannot be directly applied to human patients because of the application method (intraperitoneal injection), this study highlights the role of MSCs in sterile inflammation, such as chemical burns, and shows that they can reduce IL17-associated inflammation, in the early stages, that leads to ocular blindness. Additional studies are needed pending the development of appropriate application methods for clinical usage. Our study was limited by the indirect evidence because we negatively sorted the non-Th17 cells, and these non-Th17 cells included mixed cell populations (gammadelta T-cells, NK cells, and NK T-cells). Nevertheless, it would be noteworthy to show the effect of MSCs on the non-Th17 cells in vivo model, which could help with understanding IL-17-secreting cell changes during an adaptive immune response in an ocular chemical burn. Because of the small number of experimental sets (all the cornea were pooled, lymph node data n = 5), we could not directly determine the statistical significance and relationships in the study. However, we demonstrated the immunological profile tendencies over time and the tendency of changes in the MSCs application, which is important for future studies. Another limitation is that we used rat MSCs in the mouse study. MSC immunosuppressive properties are believed to permit allogenic or even xenogenic transplantation. Spontaneous immortalization and malignant transformation of human adipose and mouse bone-marrow-derived MSCs after in vitro culture expansion have been reported [28,29,30,31,32,33]. In contrast to the behavior of mouse cells, MSC cultures derived from rat bone marrow mononuclear cells maintained contact inhibition in culture and showed no evidence of lung tumor formation after intravenous injection into syngeneic recipients [31]. Therefore, we preferred rat MSCs rather than mouse MSCs for this study based on this reason. However, further study is needed to determine the stability and xenogenic effects of cultured rat MSCs.
In conclusion, both IL-17-secreting, non-Th17 cells and Th17 cells were involved in the ocular sterile inflammation induced by a chemical burn, and MSCs effectively suppressed the non-Th17 cells in the cornea.
Acknowledgements
This work was supported by the National Research Foundation of Korea Grant funded by the Korean Government (MEST) (NRF 2010-0010629 and NRF 2011-0004128).
Notes
No potential conflict of interest relevant to this article was reported.