

Ocular adnexal lymphoproliferative lesions are lymphohistologic masses that can appear in various locations, including the conjunctiva, orbit, eyelid, lacrimal duct, and lacrimal gland. They can be both primary or secondary and encompass a wide disease spectrum ranging from benign lymphoid hyperplasia (BLH) to malignant lymphoma. Conjunctival lymphoproliferative lesions have the best prognosis among ocular lymphoproliferative lesions; the majority are diagnosed as BLH. It has been reported that more than 90% of such lesions do not go on to develop into systemic lymphoma [1]. There is no definitive recommended treatment for conjunctival BLH, but reported treatments include cryotherapy and the combination of surgical excision and oral steroid administration [2,3]. There have also been reports of using local radiotherapy to prevent malignant proliferation and systemic invasion [4]. However, cryotherapy or surgical excision carry the risk of cosmetic problems due to scar formation. Furthermore, localized radiotherapy, cryotherapy, or surgical excision would be difficult to perform in lesions with limbal neovascularization. As such, we report the first case of conjunctival BLH treated with bevacizumab injection.
Case Report
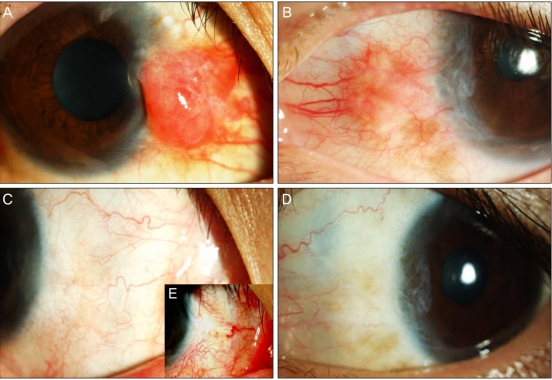
A 27-year-old man with a two year history of bilateral medial conjunctival masses was referred to our hospital. His chief complaint was injection of both eyes. His best corrected visual acuity was 20/20 and the intraocular pressures in both eyes were within normal limits. Color vision testing, automated visual fields, fundus examination, and extraocular muscle function were normal bilaterally. There were no palpable masses or edema in the eyelids and there was no exophthalmos. Slit lamp examination revealed a protruding hypervascular mass with combined medial limbal neovascularization on each medial conjunctival surface. Specifically, examination revealed a salmon colored, elevated (2 mm), moderately firm patch (6 mm ├Ś 5 mm) on the nasal conjunctiva of the right eye with neovascularization. A faint, salmon colored, elevated (1 mm) mass (5 mm ├Ś 4 mm) on the nasal conjunctiva of the left eye, with thinner new vessels than in the right eye, was also observed (Fig. 1A and 1B).
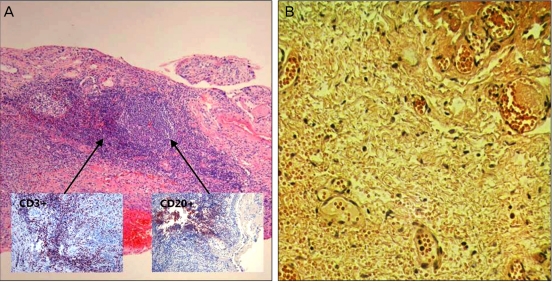
Incisional biopsy was performed on the mass in the right eye for definitive diagnosis. Pathological examination revealed benign lymphohistiocytic infiltrates (Fig. 2). The lymphoid reaction showed T cells (CD3+) and B cells (CD20+) with no evidence of atypical malignant cells. The patient subsequently underwent a complete physical exam, including serology (thyroid function tests) and radiology (chest radiography and abdominal unltrasonography), to rule out systemic disease. There were no significant findings.
Given the combination of BLH with hypervascular masses and medial limbal neovascularization, bevacizumab (2.5 mg / 0.1 mL) (Avastin; Genentech, South San Francisco, CA, USA) was injected into both medial subconjunctival spaces. Two months after injection, both masses had almost completely disappeared and the accompanying neovascularization was reduced (Fig. 1D and 1E). The patient did not experience recurrence or any other complications during the one-year follow-up period.
Discussion
Appropriate treatment for ocular BLH remains controversial. Many physicians simply recommend observation. The reported treatments for orbital BLH include surgical excision, radiation therapy, systemic corticosteroid treatment, chemotherapy, and cryotherapy. Chemotherapy can be used for lymphoma in the conjunctiva if it coexists with systemic lymphoma. One report found the final remission rate to be 98% for cryotherapy used to treat lymphoma localized in the conjunctiva [5]. Additionally, local excision or oral or topical corticosteroids can also be considered as treatment options. However, in the present case, localized radiotherapy, cryotherapy, or surgical excision would have been inappropriate treatment options because the lesion was accompanied by limbal neovascularization and surgical excision carries the risk of postoperative cosmetic defects. As such, bevacizumab injection was administered under the assumption that the conjunctival BLH, which is often difficult to treat using existing treatment methods, could be treated by altering the ocular surface blood vessels and lymphatic vessel formation.
Bevacizumab is an anti-vascular endothelial growth factor (VEGF)-A antibody approved to treat metastatic colorectal cancer [6]. Recently, it has been reported that anti-VEGF antibody may be effective in treating age-related macular degeneration and diabetic retinopathy [7,8]. Bevacizumab has recently been studied as a treatment option for neovascularization in ocular surface diseases [9-11]. However, it is unclear if bevacizumab inhibits lymphangiogenesis. Only a handful of experimental approaches deal with the inhibition of lymphangiogenesis (e.g., the use of VEGFR1R2-Trap [12] or a blocking anti-VEGFR3-antibody [13]). Recently, several studies have reported that VEGF-A not only mediates hemangiogenesis, but also lymphangiogenesis [14-16]. Given this, bevacizumab has been reported to be an inhibitor of angiogenesis and lymphangiogenesis on the ocular surface [17]. According to this report, bevacizumab also inhibits the proliferation of lymphatic endothelial cells. However, there has not yet been a report of conjunctival BLH treated with bevacizumab.
In this case, we hypothesized that with the inhibition of new blood and lymphatic vessel formation due to bevacizumab injection, the influx of polyclonal lymphocytes would be blocked and the polyclonal lymphocytes that had already accumulated would be drained by the existing lymphatic vessels. We subsequently observed a dramatic response to the local subconjunctival injection of bevacizumab. The bevacizumab near the reactive follicle must have been sufficient to suppress the inflow of lymphocytes. In the treatment of BLH, a common lymphoma in the conjunctiva, subconjunctival injection of bevacizumab can be a useful treatment option for patients who cannot tolerate a surgical procedure because of limbal neovascularization.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






