Estrogen Antagonist and Development of Macular Hole
Article information
Abstract
To describe the clinical and optical coherence tomography (OCT) features of a macular hole (MH) or its precursor lesion in patients treated with systemic antiestrogen agents. We reviewed the medical history of the patient, ophthalmic examination, and both fundus and OCT findings. Three female patients receiving antiestrogen therapy sought treatment for visual disturbance. All of the patients showed foveal cystic changes with outer retinal defect upon OCT. Visual improvement was achieved through surgery for the treatment of MH in two patients. Antiestrogen therapy may result in MH or its precursor lesion, in addition to perifoveal refractile deposits. OCT examination would be helpful for early detection in such cases.
Tamoxifen is an oral nonsteroidal antiestrogen drug which is most commonly used at low dosages (20 mg daily) for the adjuvant treatment of breast cancer [1]. Toremifen is a triphenylethylene derivative which was developed in an effort to improve the therapeutic-to-toxic ratio of tamoxifen. Tamoxifen has proven to be relatively free of serious adverse effects, but some retinal abnormalities have been reported-most notably refractile perifoveal opacities, cystoid macular edema, and retinal pigment epithelial abnormalities [1,2]. While some cases of the formation of macular holes (MH) in association with tamoxifen have been reported [3,4], as of yet, there has been no report addressing the formation of MH in a patient taking toremifen. In this study, we describe three cases of MH or its precursor lesion in patients treated with systemic antiestrogen agents.
Case Report
Case 1
A 36-year-old woman was referred to our clinic with a diagnosis of foveal cyst OU, which were detected upon fundus examination in June 2005. The patient had complained of decreased vision for several months. Her past medical history included a radical mastectomy for breast carcinoma in March 2003. After mastectomy, she had been started on toremifen, at a daily dose of 40 mg. Her visual acuity (VA) was 20/32 OD and 20/70 OS. No anterior segment abnormalities were detected. Fundus examination revealed cystic changes in the foveal center OU (Fig. 1A and 1B). Optical coherence tomography (OCT) showed a focal defect of the outer retinal layer OU (Fig. 1C and 1D). She was diagnosed with symptomatic impending MH (Gass, stage Ib). In July 2005, her left eye was treated via pars plana vitrectomy, internal limiting membrane (ILM) peeling, and SF6 gas tamponade, after obtaining informed consent. The MH was successfully closed (Fig. 1F). In October 2005, fundus examination revealed aggravated cystic changes in the foveal center OD. Her VA was 20/125 OD and 20/32 OS at that time. An OCT scan of her right eye revealed an enlarged outer retinal defect (Fig. 1E). Her right eye was also treated via pars plana vitrectomy, ILM peeling, and SF6 gas tamponade. She had discontinued her toremifen regimen in October 2005. In January 2006, a fundus examination and OCT scan revealed the successful closure of the holes OU (Fig. 1G and 1H), and her VA was improved to 20/30 OD and to 20/25 OS.
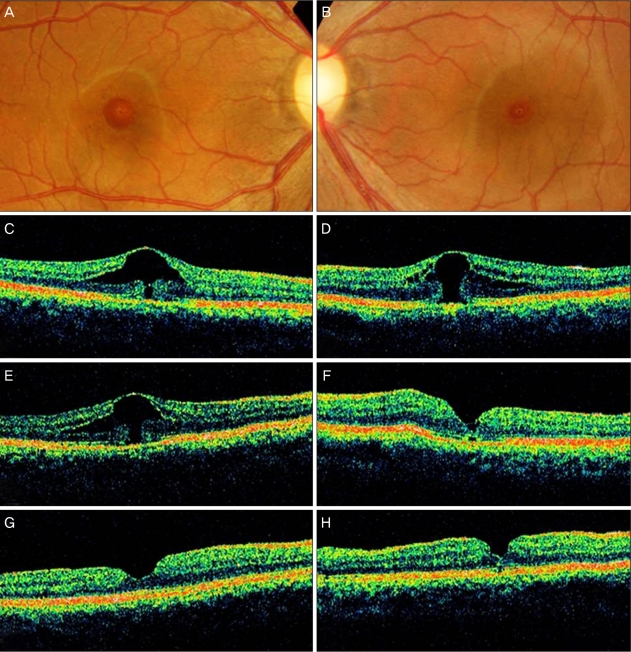
Fundus photograph and optical coherence tomographic images of both eyes of patient 1. (A,C) At presentation, the image shows foveal cystic changes with outer retinal defect in the patient's right eye. (B,D) At presentation, the image shows a stage 1b macular hole in the left eye. (E) The enlargement of outer foveal defect is noted in the right eye 4 months after initial presentation, with further deterioration of vision. (F) However, improved foveal contour and vision is noted after macular hole surgery in the left eye. (G,H) The closure of macular hole is achieved in both eyes after completing the surgery in both eyes.
Case 2
A 59-year-old woman was examined with a complaint of a six-month history of progressive visual loss and central scotoma OD. Four years ago, she had undergone a radical mastectomy for breast carcinoma. She was treated with a cumulative dose of 55 g toremifen over 46 months after surgical resection. VA was 20/125 OD. Fundus examination of her right eye revealed a cystic change in the foveal center (Fig. 2A). Additionally, a focal defect of the outer retinal layer was noted on OCT examination (Fig. 2B). Surgery for the treatment of MH was conducted two weeks after her initial visit. The MH was sealed, resulting in an improvement of VA to 20/63 (Fig. 2C).

Right eye of patient 2. Fundus photographic image (A) shows foveal cystic change, and the optical coherence tomographic image (B) shows a focal outer retinal defect at initial presentation. The contour of the fovea returns to normal after macular hole surgery.
Case 3
A 51-year-old woman had a chief symptom of decreased VA OS, which had developed several months ago. In November 2008, she was referred to us due to a macular abnormality. In February 2001, she underwent a modified radical mastectomy for invasive ductal cancer (T2N0M0, stage IIa). She was also treated with 2.5 mg tamoxifen on a daily basis from April 2007 to March 2008. She has discontinued her tamoxifen regimen due to vaginal bleeding. Upon examination, VA was 20/20 OD and 20/30 OS. Fundus examination showed refractile deposits in both macular areas (Fig. 3A and 3B). OCT showed a normal OD; however, a focal defect of the outer retinal layer was observed in the fovea OS (Fig. 3C and 3D). Additionally, the patient has been put on a follow-up schedule of regular 3-month intervals. In April 2009, we noted no changes in the OCT findings OU (Fig. 3E).
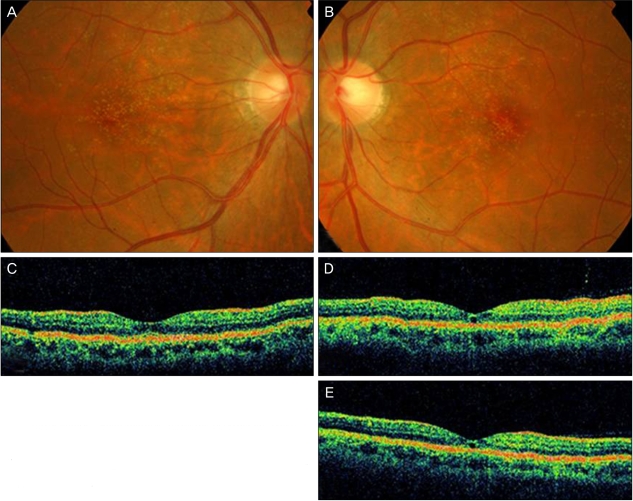
Fundus photographic images of both eyes in patient 3. At initial presentation, small multiple refractile deposits are noted in both of the patient's eyes (A,B). Optical coherence tomographic (OCT) scan of the macula shows no specific abnormality in the right eye (C); however, a focal defect of the outer retinal layer is noted in the left eye (D). No interval change in OCT findings is noted after 5 months (E).
Discussion
All patients referenced herein experienced visual disturbances associated with MH precursor lesions. Additionally, visual improvements were achieved via MH surgery. Although previous reports of ocular abnormalities have raised some concerns regarding antiestrogen use, significant deterioration of vision is rare, at least in cases of short-term administration.
Idiopathic MH occurs predominantly in old women (74%) [5]. Case 2 coincided with the demographic profile of idiopathic MH. Furthermore, the lesion developed unilaterally in this case. Thus, it remains uncertain as to whether there was a real association with the administration of antiestrogen agents. However, case 1 was much younger than the idiopathic MH patients, and evidenced bilateral involvement. Additionally, in case 3, typical refractile deposition was noted in both eyes, along with unilateral MH precursor lesion.
The mechanisms of MH formation following administration of an antiestrogen agent are merely speculative. It is worth noting that idiopathic MHs predominantly occur in postmenopausal women, and current estrogen users were found to be at reduced risk for developing MH [6]. Elevated serum fibrinogen levels have been noted in menopausal women and may induce a rapid deceleration of blood flow in the submacular choroid, eventually rendering foveal tissue susceptible to vitreous traction [6]. As our patients were treated with antiestrogen agents over a long period, the development of MH precursor lesions would be related to their depleted plasma estrogen.
In one report of eyes evidencing tamoxifen retinopathy, foveal cystoid space and the interruption of the photoreceptor line, observed upon OCT, was described [2]. It remains uncertain as to whether the case was actually representative of an MH precursor lesion. In another report, MH in 4.12% of female patients were associated with current use of tamoxifen [3]. The natural course of MH or its precursor lesion after systemic antiestrogen administration remains unknown. However, recognizing the development of MH appears worthwhile, because, as was noted in our cases, vision can be restored via surgical intervention. Physicians should be aware of and concerned about this retinal complications. Periodic OCT examinations after the systemic administration of antiestrogen, especially in cases in which the patient complains of visual deterioration or metamorphopsia, would be helpful for early identification.
Notes
No potential conflict of interest relevant to this article was reported.