


Silicone tube intubation is the primary treatment for treatment of nasolacrimal drainage disorder. The indications for silicone tube intubation include punctal or lacrimal canalicular and nasolacrimal duct stenosis associated with allergic conjunctivitis, recurrent viral conjunctivitis, or anti-cancer medication [1,2]. The tube is usually removed from the duct 6 months after intubation. Many factors affect the success rate of silicone tube intubation, such as biofilm-related infection, early silicone tube prolapse, or the preoperative condition of the lacrimal duct [3,4]. The cause of early silicone tube prolapse can be a surgeon-related factor such as inappropriate length of the silicone tube, but is more often to do with careless rubbing by the patient immediately after surgery. Therefore, including in some congenital nasolacrimal duct obstruction cases, ST fixation at the nasal mucosa using 6-0 Prolene or silicone sponge technique can be used to prevent early tube prolapse [5,6]. Recent studies by Chu et al. [7] and He et al. [8] describe methods that can be used to reposition the prolapsed silicone tube using a suture-probe or a memory wire probe, respectively. Herein, we present a new, effective hole and lacrimal probe method for repositioning the prolapsed silicone tube using lachrymal probe, drop-shaped tip, size 0000-000, stainless steel (D-110S; Cilita, Ryazan, Russia) without local anesthesia.
Materials and Methods
The analysis was performed in adherence with the Declaration of Helsinki and after approval from the institutional review board and ethics committee of the HanGil Eye Hospital in Incheon, Korea. Because this study is a retrospective analysis of clinical data, we submitted a reason for exemption in written informed consent to institutional review board. From January 2019 to February 2021, all patients had been treated with bicanalicular silicone tube intubation for treatment of stenosis of punctum in four cases, stenosis of the punctum and canaliculus in two cases, stenosis of the punctum and nasolacrimal duct in three cases, and stenosis of canaliculus and nasolacrimal duct in two case. And 10 patients were decided to have the conjunctivoplastic surgery for the treatment of conjunctivochalasis. All patients enrolled in this study demonstrated prolapse of silicone tube at medial canthus but the tube was not visible in the inferior meatus under nasal endoscopy and thus could not be repositioned through nasal cavity in HanGil Eye Hospital. The tube dislocation occurred 1 day to 8 weeks after the first surgery. The cause of silicone tube prolapse was rubbing by the patients after initial intubation.
The procedure uses lachrymal probe, drop-shaped tip, size 0000-000, stainless steel (D-110S, Cilita). All patients underwent immediate reposition of prolapsed silicone tube using our new method without local anesthesia in the outpatient operating room.
First, the prolapsed silicone tube is held in a half circle and cut obliquely using Vannas scissors, not cutting completely (Fig. 1A). Subsequently, a small semicircular hole is created in the silicone tube (Fig. 1B). The probe is inserted into the hole in the silicone tube (Fig. 1C). After proparacaine eye drops are applied, the probe already inserted through the hole into the silicone tube is carefully inserted into the Hasnerâs valve, as in the first operation (Fig. 1D). The probe in the silicone tube can be seen from Hasnerâs valve under nasal endoscopy (Fig. 1E). Finally, after the silicone tube from Hasnerâs valve is caught by Ritleng forceps, the probe is pulled back out from the upper punctum, with the result that the prolapsed silicone tube is well repositioned (Fig. 1F). The knot portion of the silicone tube is properly repositioned in the inferior meatus using Bayonet dressing forceps.
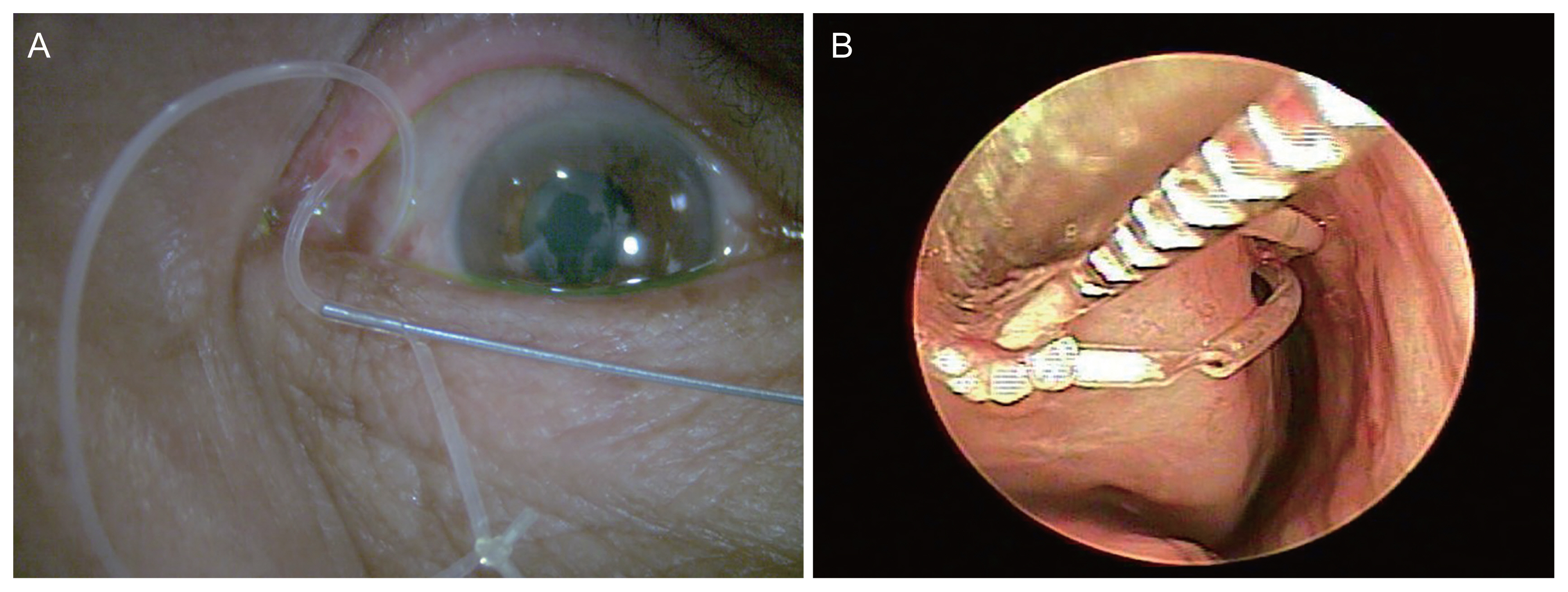
If the knot of the prolapsed silicone tube could be seen outside, it is important to make the hole close to the knot and insert probe in the opposite direction of the knot into the hole so that the probe can be allowed to enter the punctum first and then the knot to fellow through the punctum (Fig. 2A). The next procedure is the same as above mentioned. At the 3-month follow-up, the silicone tube was well positioned without break around the hole on nasal endoscopic examination (Fig. 2B).
Results
In all patients (five males and six females), the prolapsed silicone tube was successfully repositioned using this hole and lacrimal probe method without any complications. The mean age of all patients was 61.4 years (range, 14-82 years). The tube was never completely cut or broken during the insertion of the lacrimal probe into the hole made in the tube.
After silicone tube reposition, oral antibiotics for 3 days and antibiotic eye drops for 2 weeks were prescribed. Until extubation, all patients visited the hospital every month to check the condition of the tube using a nasal endoscope. At 6-month follow-up examination after initial intubation, all the patients presented with a well-positioned silicone tube without break around the hole on nasal endoscopic examination.
Discussion
Repositioning a prolapsed silicone tube which is not visible at the inferior meatus is very complicated. A prolapsed silicone tube after dacrycystorhinostomy surgery may be repositioned more simply, as the tube is easily visible through the rhinostomy site [9]. When a prolapsed tube is hard to reposition it may be removed at an early stage, resulting in lower success rate for nasolacrimal duct stenosis [10,11]. Chu et al. [7] reported that repositioning of the dislocated silicone tube was successful using suture-probe technique. He et al. [8] introduced a technique that uses memory wire probe and nylon to make a suture knot in order to capture the dislocated silicone tube. The above methods were both performed under local anesthesia and required special probes. Herein, we present a new technique that uses a Hole and lacrimal probe. A small hole is made to the prolapsed tube using Vannas scissors, and then after the probe is inserted into the hole, the engaged probe with the silicone tube is passed through the lacrimal sac and nasolacrimal duct. Finally, Bowman probe engaged with the tube can be seen over the Hasnerâs valve. In contrast to the reports of recent researches, the lacrimal probe is inserted into the hole of the prolapsed silicone tube and then into the lacrimal duct, so there is little risk of damaging the tissues of the lacrimal duct.
The advantages of this method are that the patient feels no pain during the making of a hole at the prolapsed silicone tube and the insertion of the lacrimal probe into the hole because the process is taken place at the prolapsed tube. Moreover, the whole process can be performed under topical anesthesia in the outpatient operating room. Some methods for preventing the early prolapse of silicone tube have been presented, including nasal fixation with suture or sponge [5,6]. However, due to its complexity, surgery has usually been completed by tying the two free ends of each tube instead of nasal fixation of the silicone tube. The rate of early silicone tube prolapse in children has been reported as 17.5% to 44%, which has a critical effect on the surgical outcome [12,13].
Opinions may still be divided on whether to reposition the prolapsed silicone tube or insert a new one after removal of prolapsed tube. In our cases, however, the tubes were all prolapsed in a relatively short time after lacrimal intubation due to rubbing by patients, and since there was no change on the tubes to the extent that biofilm was produced, the prolapsed tubes were repositioned without considering re-inserting new tube. So that we didnât need to replace it with a new silicone tube.
The limitation of this method is that while it is feasible for repositioning a dislocated hollow silicone tube after bicanalicular intubation, its use is limited with a solid core silicone tube.
In conclusion, Hole and Lacrimal Probe method is effective for the repositioning of prolapsed silicone tube after bicanalicular intubation of lacrimal system.

 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






