

Glaucoma drainage valves can be implanted to reduce intraocular pressure (IOP) in eyes with intractably elevated IOP [1,2,3,4]. Such treatment is usually preferred when conventional trabeculectomy is likely to fail or has failed already. For instance, glaucoma drainage valves are often implanted to treat elevated IOP in eyes that have undergone pars plana vitrectomy (PPV) [5,6,7]. IOP might be elevated due to either to the PPV procedure or the ocular pathology that prompted the PPV [8,9,10]. Up to 35% of patients who undergo PPV subsequently experience IOP elevation to higher than 30 mmHg [8]. When IOP is elevated shortly after PPV, it may soon resolve; however, in some eyes, IOP remains high and must be lowered surgically. Although glaucoma drainage valves are commonly implanted in eyes with elevated IOP after PPV, no research has thoroughly investigated the factors associated with long-term outcomes of this treatment. Therefore, we analyzed the outcomes of Ahmed glaucoma valve (AGV) implantation in eyes with intractably elevated IOP after PPV. Furthermore, we explored which factors were associated with these long-term outcomes. In particular, we investigated various factors associated with PPV procedures themselves as well as preand post-PPV ocular status.
Materials and Methods
Subjects
Data were retrospectively collected from consecutive patients who underwent AGV implantation (model: FP7) after PPV at the glaucoma clinic of Asan Medical Center, Seoul, South Korea, between March 2008 and July 2014 to treat intractable IOP elevation. In all patients, IOP remained high, although the maximum-tolerated medical therapy (MTMT) was used. All AGVs were implanted by a single surgeon (KRS). Only patients who had been followed up for at least 1 year after implantation were included. If both eyes from a single patient met the inclusion criteria, one eye was chosen at random. Patients who underwent concomitant procedures, such as cataract extraction, penetrating keratoplasty, or silicone oil (SO) removal, during AGV implantation were excluded. Eyes that showed rubeosis at either the anterior chamber angle or the iris before PPV, i.e., diagnosed as neovascular glaucoma (NVG) before PPV were also excluded. The study was approved by our institutional review board (2016-0507) and followed the principles of the Declaration of Helsinki. Written informed consent was obtained.
Surgical procedure
The surgical procedure has been described elsewhere [11]. Briefly, AGVs were implanted by using a fornix-based conjunctival flap, which was constructed at the superotemporal or inferotemporal area. A limbus-based, half-thickness scleral flap (5-mm circumference ├Ś 7-mm radius) was then prepared. The AGV was placed under Tenon's capsule, 8 to 10 mm posterior to the superotemporal or inferotemporal limbus. It was fixed and sutured with a 9-0 nylon suture. The chamber was accessed under the scleral flap with a 23-gauge needle, and the AGV was implanted 2 mm posterior to the limbus, parallel to the plane of the iris. The tube was inserted in the bevel-up position into the anterior chamber. The scleral flap was sutured with 9-0 nylon, and a watertight conjunctival closure was performed. A topical corticosteroid, cycloplegic, and antibiotic were prescribed for approximately 1 month after surgery, though the length of prescription depended on the condition of the eye. If severe rubeosis was observed in the iris or anterior chamber angle before AGV implantation, anti-vascular endothelial growth factor (anti-VEGF) was injected intracamerally. Follow-up examinations were performed 1 day, 1 week, 1 month, and 6 months after surgery and every 6 months thereafter. Additional visits were scheduled as needed.
Analysis
At each visit, IOP was measured by Goldmann applanation tonometry, and the attending physician noted whether IOP-lowering medication was being used. Any complications were recorded. The surgery was considered a success if IOP was 6 to 21 mmHg, regardless of whether IOP-lowering medication was being used, but without additional glaucoma surgery, AGV removal, or serious complications.
The following variables were compared between the ŌĆ£successŌĆØ and ŌĆ£failureŌĆØ groups: pre-PPV diagnosis, presence of diabetes mellitus (DM), glaucoma diagnosis before PPV, best-corrected visual acuity, presence of peripheral anterior synechiae greater than 180 degrees of the anterior chamber angle, presence of rubeosis at either the anterior chamber angle or iris before AGV implantation, lens status at AGV implantation, presence of SO, interval between PPV and AGV implantation, PPV before IOP, IOP 1 week after PPV, mean and peak IOP in the interval between PPV and AGV implantation, and duration of MTMT before AGV implantation. Variables related to the PPV procedure were also compared between groups, namely PPV operation time, concurrent phacoemulsification, concurrent scleral buckling (segmental or encircling buckle), and vitrectomy probe size (20G, 23G, and 25G). History of anti-VEGF injection or concurrent anti-VEGF injection at AGV implantation was also assessed. IOP was measured and compared 1 week, 1 month, and every 6 months after AGV implantation. The Kolmogorov-Smirnov test was used to test for the normality of numeric variables. To compare two normally distributed numerical variables, an unpaired t-test was used. Chi-squared tests were performed to compare categorical data. Univariate and multivariate Cox proportional hazard modeling was conducted to determine which factors were associated with failed AGV implantation. This modeling included the aforementioned putative factors as well as demographics. Variables with a p-value <0.3 in univariate analyses were included in multivariate analyses. To ensure that highly correlated variables do not affect each other in multivariate analyses, only peak IOP values during each period (before PPV, PPV-AGV, and after AGV) were included in the multivariate model. The same analyses were performed with subgroups that had rubeosis before AGV implantation (NVG group) and that underwent AGV implantation within 100 days after PPV (early AGV group). All statistical analyses were performed with IBM SPSS Statistics ver. 24.0 (IBM Corp., Armonk, NY, USA).
Results
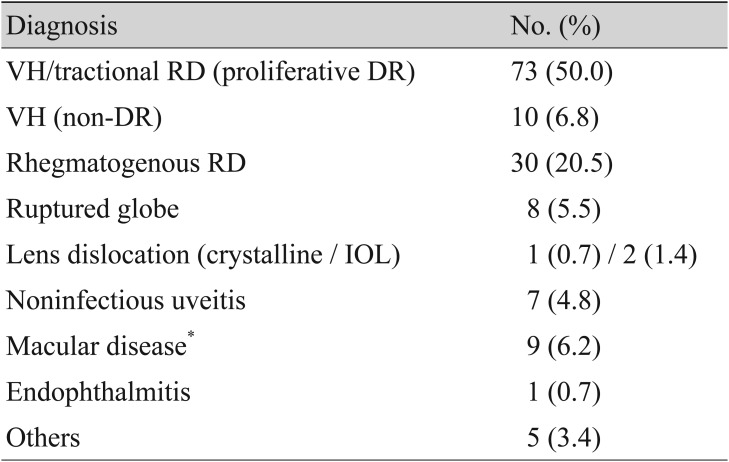
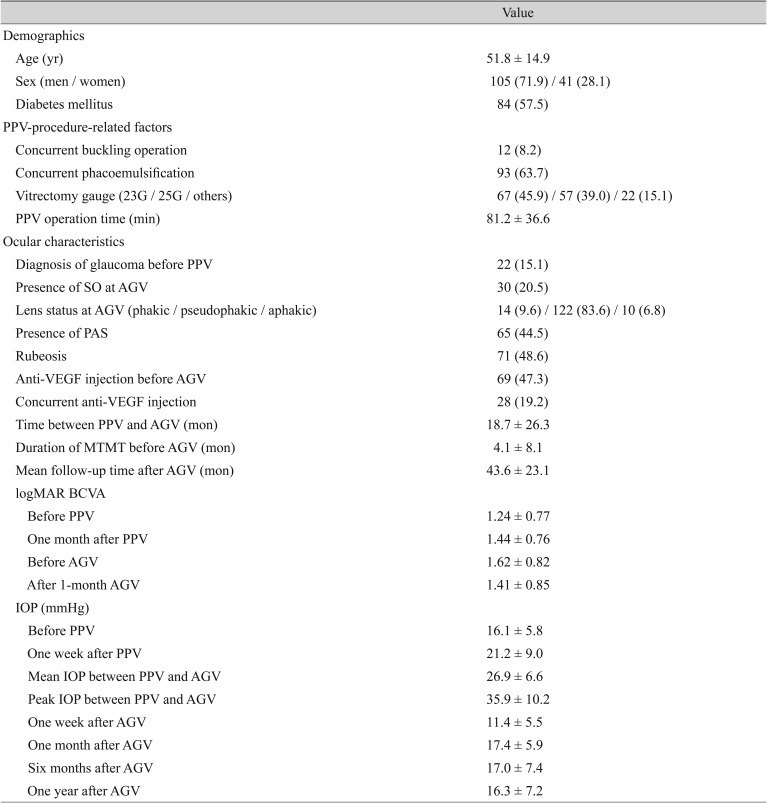
A total of 146 eyes from 146 patients were included in the final analyses. This group included 105 men and 41 women; all were Asians (1 Indonesian and 145 Koreans). The mean (┬▒ standard deviation) age at AGV implantation was 51.8 ┬▒ 14.9 years. The most common cause of PPV with subsequent AGV implantation was proliferative diabetic retinopathy (PDR) that led to vitreous hemorrhage or traction retinal detachment (73 eyes, 50.0%) followed by rhegmatogenous retinal detachment (30 eyes, 20.5%). Trauma-related globe rupture and non-diabetic vitreous hemorrhage accounted for 8 and 10 cases, respectively (Table 1).
The mean IOPs before and 1 week after PPV were 16.1 ┬▒ 5.8 and 21.2 ┬▒ 9.0 mmHg, respectively. The mean and peak IOPs between PPV and AGV implantation were 26.9 ┬▒ 6.6 and 35.9 ┬▒ 10.2 mmHg, respectively. The mean duration of MTMT before AGV implantation was 4.1 ┬▒ 8.1 months. The mean elapsed time between PPV and AGV implantation was 18.7 ┬▒ 26.3 months. Among the 146 eyes, peripheral anterior synechiae was observed in 65 (44.5%) and rubeosis in 71 (48.6%) before AGV implantation (Table 2).
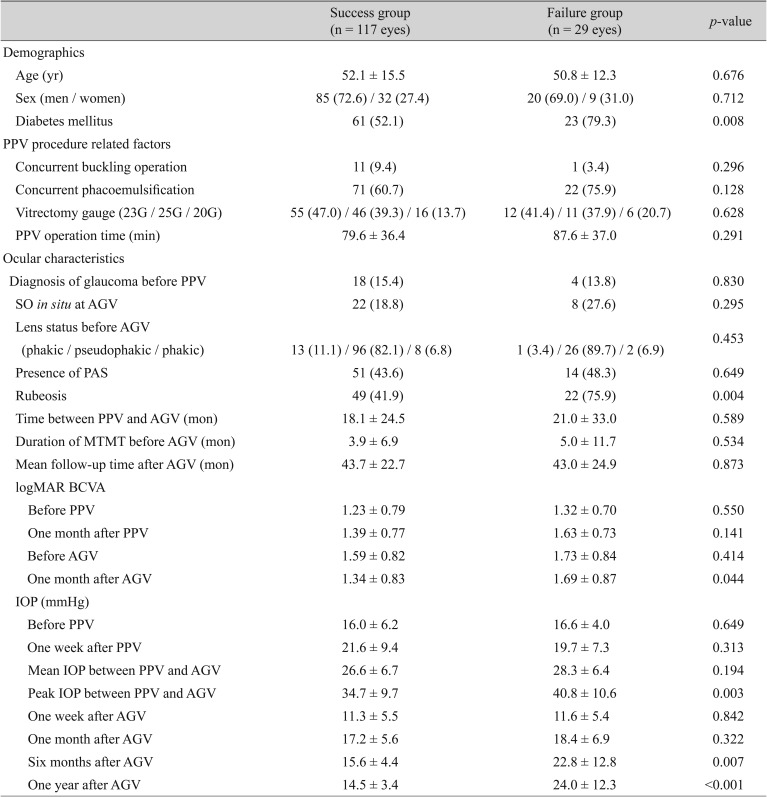
The mean follow-up period after AGV implantation was 43.6 ┬▒ 23.1 months. Overall, 117 eyes (80.1%) were categorized as ŌĆ£successfulŌĆØ at last follow-up. The ŌĆ£failureŌĆØ group consisted of 29 eyes: 23 of which had an IOP higher than 22 mmHg despite medical treatment and 6 had hypotony (IOP lower than 6 mmHg). Among the 29 eyes in the ŌĆ£failureŌĆØ group, 3 underwent additional AGV implantation. The ŌĆ£successŌĆØ and ŌĆ£failureŌĆØ groups did not differ significantly in terms of age, sex, or IOP before, 1 week after, or 1 month after PPV. However, peak IOP before and 6 months after AGV were higher in the ŌĆ£failureŌĆØ group (34.7 ┬▒ 9.7 vs. 40.8 ┬▒ 10.6 mmHg, p = 0.003; 15.6 ┬▒ 4.4 vs. 22.8 ┬▒ 12.8 mmHg, p < 0.007; respectively (Table 3). The DM prevalence was significantly greater in the ŌĆ£failureŌĆØ group (79.3%) than in the ŌĆ£successŌĆØ group (52.1 %), and rubeosis was more common before AGV implantation in the ŌĆ£failureŌĆØ group (75.9%) than in the ŌĆ£successŌĆØ group (41.8%). No PPV-related factors were differed significantly between groups (Table 3).
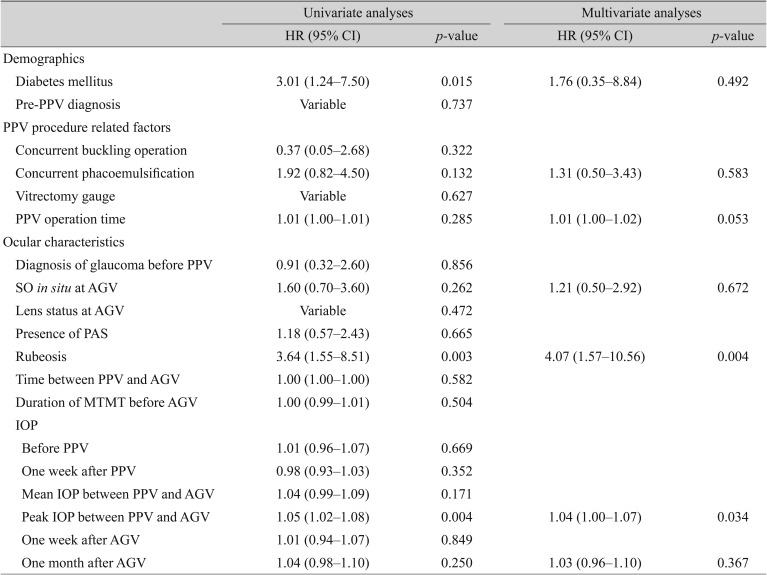
Among the factors associated with failed AGV implantation, univariate analyses revealed that the presence of DM, peak IOP between PPV and AGV implantation, and the presence of rubeosis were possibly associated. In multivariate analyses, rubeosis and peak IOP were predictive of surgical failure (hazard ratio [HR], 4.07; 95% confidence interval [CI], 1.57 to 10.56; p = 0.004; HR, 1.04; 95% CI, 1.00 to 1.07; p = 0.034; respectively) (Table 4). No PPV-procedure-related variables were associated with longitudinal outcomes after AGV implantation.
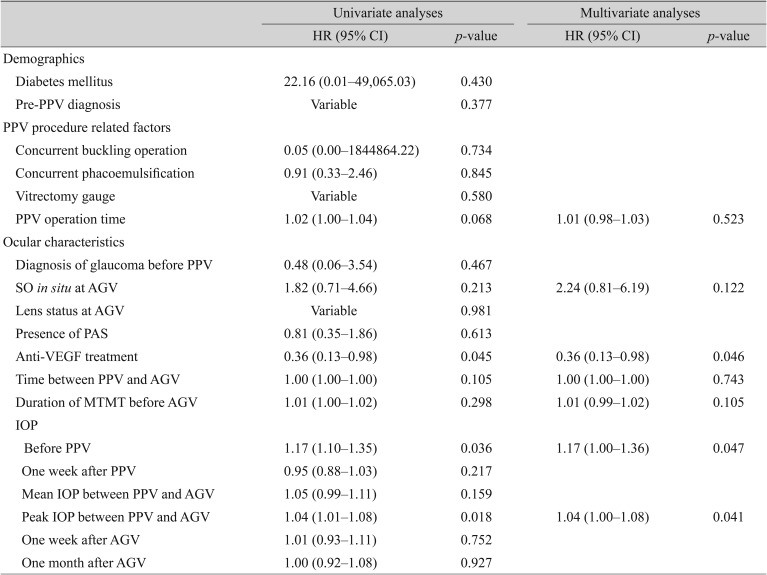
Subgroup analyses were performed for the 71 NVG eyes that had rubeosis before AGV implantation. Either pre-AGV intravitreal anti-VEGF injection or concurrent intracameral anti-VEGF injection at AGV implantation were more common in the ŌĆ£successŌĆØ group than in the ŌĆ£failureŌĆØ group (93.9% [46 / 49] vs. 77.3% [17 / 22], p = 0.041). This result was confirmed in the Cox analysis showing that anti-VEGF injection was predictive of long-term success (HR, 0.36; 95% CI, 0.13 to 0.98; p = 0.046) (Table 5). IOP before PPV and peak IOP before AGV were also associated with surgical failure in this subgroup (HR, 1.17; 95% CI, 1.00 to 1.36; p = 0.047; HR, 1.04; 95% CI, 1.00 to 1.08; p = 0.041; respectively) (Table 5).
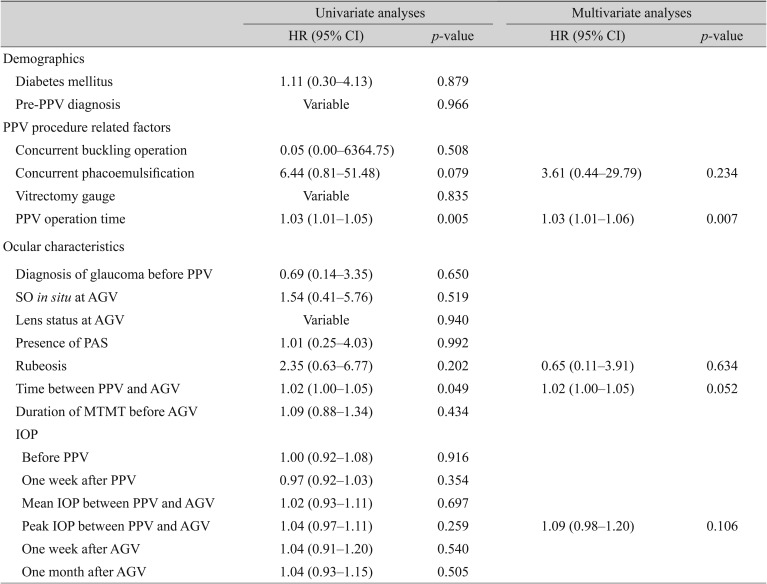
Additional subgroup analyses were performed for the 38 eyes that underwent AGV implantation within 100 days of PPV. The percentage of eyes with an initial diagnosis of ruptured globe or macular disease was 10.5% (4 / 38), but the percentage with DMR was similar to that for the total study population (47.4% vs 50.0%). Rubeosis and peak IOP between PPV and AGV were not significant factors for failed AGV implantation, but PPV time, concurrent phacoemulsification at PPV, and elapsed time between PPV and AGV showed a possible association. In multivariate analyses, however, only PPV time was statistically significantly associated with the long-term success of AGV implantation (HR, 1.03; 95% CI, 1.01 to 1.06; p = 0.007), and elapsed time between PPV and AGV showed a marginal association (HR, 1.02; 95% CI, 1.00 to 1.05; p = 0.052) (Table 6).
Discussion
Among eyes that had previously undergone PPV and had intractably elevated IOP despite MTMT, the overall success rate of AGV implantation was 80.1% during a mean follow-up period of 3.6 years. The mean IOP 1 year after AGV implantation was 16.3 ┬▒ 7.2 mmHg. These results are comparable to those of AGV implantation in general refractory glaucoma [2]. Taken together with previous findings, our data suggest that AGV implantation provides good surgical outcomes in eyes that have previously undergone PPV [12,13,14,15].
Eyes that had elevated IOP after PPV did not have high IOP before PPV (mean, 16.1 ┬▒ 5.8 mmHg). Nonetheless, 1 week after PPV, mean IOP increased to 21.2 ┬▒ 9.0 mmHg, which means that the majority of eyes that required AGV implantation had mild IOP elevation soon after PPV. Meanwhile, factors related to surgical procedure, such as a concurrent buckling procedure, different vitrectomy gauges, and PPV operation time, did not differ significantly between the ŌĆ£successŌĆØ and ŌĆ£failureŌĆØ groups. A similar result was found in Cox proportional hazard analysis, showing that no procedure-related factors were significant associated with outcomes of AGV implantation. In summary, the ŌĆ£failureŌĆØ group did not differ from the ŌĆ£successŌĆØ group in terms of the PPV procedure. This finding may have resulted from the variable time intervals between PPV and AGV implantation (18.7 ┬▒ 26.3 months). Patients who underwent AGV implantation a long time after PPV may have been less affected by PPV procedures. Hence, we performed a subgroup analysis of participants who underwent AGV implantation less than 100 days after PPV. The subgroup analysis found somewhat different results than the overall data showing that a longer PPV operation time was a significant risk factor for surgical failure. Hence, patients who underwent early AGV implantation soon after PPV may have been affected by the PPV procedure, but this subgroup had a small number of patients (38 patients) and further study is needed.
The most common cause of PPV with subsequent AGV implantation was PDR. The prevalence of both DM and rubeosis were significantly greater in the ŌĆ£failureŌĆØ group than in the ŌĆ£successŌĆØ group. Such eyes are prone to NVG due to ischemic insult, thus may also have intractably elevated IOP after PPV [16]. In a Cox proportional hazard analysis, the univariate result showed that both factors were associated with surgical failure. In multivariate analyses, both rubeosis and peak IOP between PPV and AGV were correlated with surgical failure. Considering that most patients with rubeosis receive PPV as a consequence of PDR, if rubeosis occurs after surgery in patients with DM, the likelihood of treatment failing due to NVG is high. Recently, intraocular injection of anti-VEGF has been to treat retinal ischemia. Intravitreal anti-VEGF injection in NVG patients could improve the prognosis of AGV implantation [17,18,19,20]. Our subgroup analysis of NVG patients also found that pre-AGV or concurrent intracameral anti-VEFG injection was predictive of surgical success. Intracameral anti-VEGF injection at the same time as AGV implantation may be an option for patients with severe rubeosis.
The presence of SO at AGV implantation was not a risk factor for surgical failure in this study. However, evidence on whether the presence of SO is a risk factor for surgical failure in AGV implantation is conflicting [14,15,21]. Ishida et al. [14] reported that AGV implantation can control IOP in a majority of eyes after PPV and SO injection. However, they found that the presence of SO was associated with increased risk of surgical failure in eyes treated with AGV. Likewise, Park et al. [15] reported that intraocular SO tamponade is a risk factor for failure of AGV implantation. However, their study, in contrast to ours, only included NVG after PPV. Meanwhile, Al-Jazzaf et al. [21] reported that SO-filled eyes that have not responded to medical therapy can be effectively managed by implanting a glaucoma-drainage device in an inferior quadrant.
Several limitations of our study should be noted. Since it was not prospectively designed and most of the participants were of a single ethnicity, the results should be interpreted with caution. We performed subgroup analyses of eyes that underwent AGV implantation shortly after PPV, and the results differed from the overall population showing that PPV time affected the outcome of AGV implantation. This result may suggest that longer PPV times are predictive of poor surgical outcomes in early AGV implantation; however, it should be duplicated with a larger sample size.
In summary, AGV implantation was successful in patients who had intractably elevated IOP after PPV in general. The development of rubeosis after PPV and a high peak IOP before AGV were predictive of surgical failure. PPV-procedure-related variables were not associated with long-term outcomes of AGV implantation.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






