

Dear Editor,
Bilateral congenital absence of the inferior rectus muscle (IR) is very rare, especially without craniofacial deformities or other extraocular muscle (EOM) abnormalities. To our knowledge, this is the first report of bilateral IR absence with severe A-type exotropia without other EOM abnormalities.
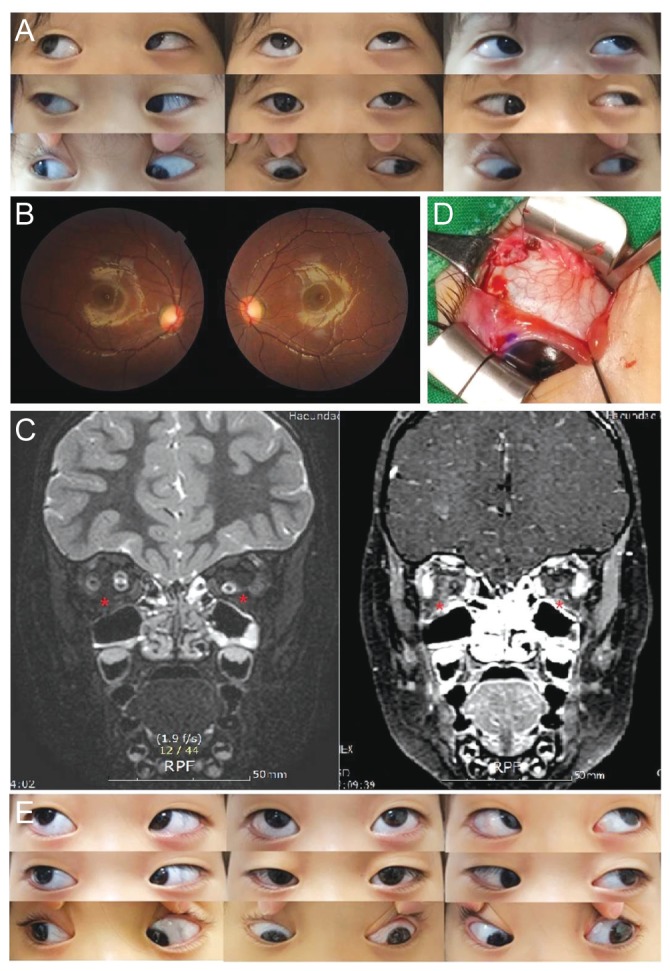
A 2-year-old girl presented with exotropia and left hypertropia (LHT) since birth. She was born at full term and had no perinatal disease, family history, or facial deformity. She had left head tilt, 30 prism diopters (PD) of hypertropia, and 30 PD of exotropia in her left eye, with the angle of exodeviation aggravated on downward gaze (A-type exotropia). She also showed 30 PD of right hypertropia on right gaze and 35 PD of LHT on left gaze. Only right hypertropia was present on left head tilt, while LHT was presented and aggravated on right head tilt. Extreme limitation of downward gaze that could not cross the horizontal midline in the left eye and -5 limitation of inferotemporal movement in both eyes were found [1] (Fig. 1A). Slit lamp examination was normal, and fundus fixation photographs showed incyclotorsion of both eyes (Fig. 1B). Orbital magnetic resonance imaging indicated bilateral absence of IR (Fig. 1C).
At age 3, she underwent bilateral lateral rectus (LR) recession 7 mm for exotropia and left superior rectus (SR) recession 7.5 mm for LHT. A forced duction test showed limitation of downward gaze due to left SR contracture. Intraoperative examination showed bilateral absence of the IR, with no other EOM abnormalities (Fig. 1D). The patient showed orthotropia in primary and upward gaze and improvement in exotropia in downward gaze and in limitation of downward movement at 1 year after the surgery (Fig. 1E). The typical manifestation of the IR absence is incomitant hypertropia in the affected eye, which becomes worse with abduction, infraduction, or head tilt to the side opposite the affected eye. Vertical deviation with unilateral IR absence was corrected by recession and anterior transposition of the inferior oblique muscle. However, recession and anterior transposition of the inferior oblique muscle may aggravate incyclotorsion, a condition frequently present in IR absence [2]. Successful surgical outcomes have also been reported in congenital left IR absence with 65 PD LHT and 48 PD exotropia [3]. Transposition of the left medial rectus (MR) and LR to the original IR insertion site and 3-mm resection of the MR resulted in vertical strabismus below 10 PD, but remaining exotropia of 22 to 25 PD. The latter was corrected by a second operation, right MR resection and LR recession. Another report described a patient with bilateral IR absence accompanied by an abnormal connection between the left inferior oblique and LR, resulting in severe limitation of ocular movement due to weakening of MR and contracture of LR [4]. For 45 PD of left exotropia and 16 PD of LHT, the patient underwent left SR recession and LR disinsertion, resulting in 12 PD of exotropia and disappearance of vertical strabismus.
For a patient with left IR absence accompanied by 35 to 50 PD of exotropia, Giller [5] performed 1) left SR recession, 2) transposition of the inferior limbs of the left MR and LR to the presumed insertion site of the IR, 3) transposition of the superior limbs of the left MR and LR to the insertion site of the inferior limbs, resection of the superior limb of the left MR, recession of the superior limb of the left LR, and 4) left inferior oblique myectomy. Although the surgical outcome was satisfactory, surgery on four EOMs was required. Horizontal muscle transposition can increase the risk of ocular ischemic syndrome in congenital IR absence because only SR remains intact after the surgery [3,4]. In most reports, even unilateral IR absence accompanied by exotropia greater than 10 PD required surgery of three EOMs in the affected eye and additional manipulation in the unaffected eye [2,5]. In bilateral IR absence, selection of surgical procedure should be considered with accompanying comorbidities. In our case, unilateral SR recession and bilateral LR recession resulted in improvements in hypertropia, exotropia, and downgaze limitation, which were sustained for 1 year after surgery. Thus, with low risk of ocular ischemic syndrome, one-step surgery on three EOMs could achieve successful outcomes in cases of bilateral IR absence with A-type exotropia.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






