

Dear Editor,
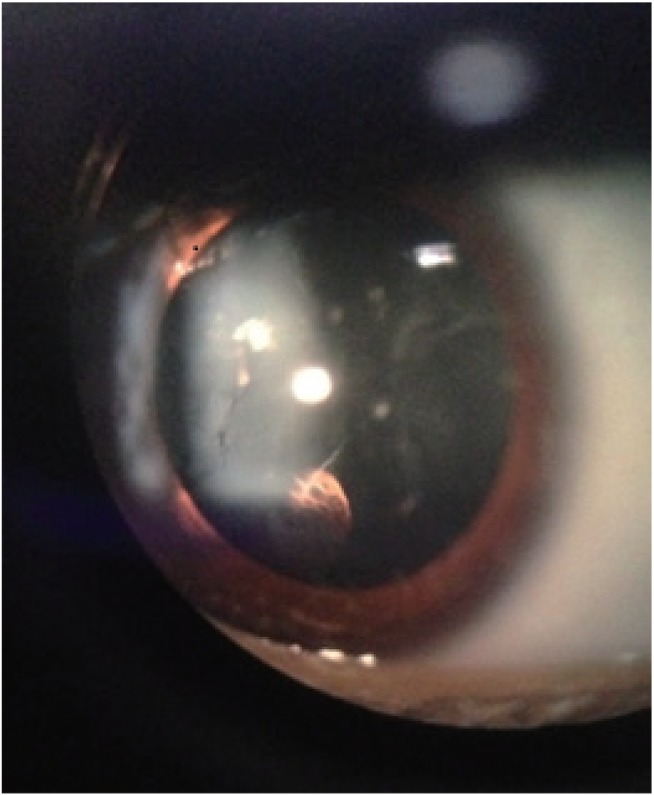
A 9-year-old female child presented with diminution of vision in both the eyes and deviation of eyes since birth. The corrected visual acuity was 1 / 60 in both eyes. There was no history of any systemic disorder or trauma. Hirschberg's test showed 20 degrees of exotropia. The prism bar covered test showed 40 prism diopter exotropia. Slit lamp examination revealed an unremarkable anterior segment with no signs of inflammation except for the presence of posterior embryotoxon in both eyes. A spherical, translucent, smooth cyst covered with a brown pigment was noted in posterior vitreous, moving freely with the movements of the eyeball in both the eyes (Fig. 1). The intraocular pressure was 16 and 15 mmHg in the right and left eye respectively.
Indirect ophthalmoscopy and biomicroscopy with 90D lens revealed a healed chorioretinitis patch in both the eyes. In the right eye, a single oval cyst was identified floating freely in the vitreous, partially masking the underlying retinal vasculature. B-scan ultrasound revealed an echogenic, round-shaped cyst measuring 2 × 1.5 mm, free from surrounding vitreous strands or retina, localized at the posterior vitreous in the right eye, and four similar miniature cysts were found in the left eye. Color doppler revealed absence of vessels passing through the vitreous of both of the globes and within the cysts. There were no signs of retinitis pigmentosa.
Indirect hemagglutinin tests for echinococcus and cysticercosis were negative. Eosinophilia was absent on peripheral blood smear. Based on these findings the patient was diagnosed with bilateral free floating vitreous cysts with posterior embryotoxon.
The first description of a vitreous cyst was by Tansley in 1899. These are classified as congenital and acquired [1]. Congenital cysts are associated with residues of the hyaloid vascular system and are occasionally seen in normal eyes. Though they may be pigmented or non-pigmented [2], they are usually non-pigmented, smooth surfaced, pedunculated or sessile and are located anterior to the optic disc. Acquired cysts are often associated with inflammation secondary to intraocular infection such as parasitic vitreitis, toxoplasmosis, uveitis, retinitis pigmentosa, choroidal atrophy and retinoschisis [3].
Age of occurrence ranges between 5 and 68 years, though majority of cases occur between 20 and 40 years of age. They may occur as a single monolateral, a single bilateral, or multiple monolaterals. Bilateral cases are usually observed in patients with retinitis pigmentosa [1].
Our patient had no history of trauma, and infection as a cause of the cysts was ruled out by negative serological tests. B-mode ultrasonography and Doppler did not show any embryonal remnants. Fundus examination showed no accompanying pathology, which has not been previously reported in the literature.
Patients are usually asymptomatic, but due to mobility of cysts, patients may complain of floaters. There is no treatment indicated for asymptomatic or mildly symptomatic cases. In symptomatic patients, the treatment options include laser photocystotomy or pars plana vitrectomy with cyst excision. Free-floating vitreous cysts, though of less clinical relevance, need to be differentiated from potentially serious conditions. Pigmented cysts can be mistaken for malignant melanoma. Grey, opaque cysts may resemble parasitic cysts as in cysticercosis. Besides clinical examination, serology for ruling out intraocular infections, ultrasonography or optical coherence tomography for detection of scolices inside the cyst were used to help reach the diagnosis.
Posterior embryotoxon is of congenital origin, and is reported to occur in otherwise normal eyes or in patients of Axenfeld syndrome, Alagille syndrome, aniridia and ocular hypertension. A higher prevalence in the younger age group of 22.5% is observed compared with 5.9% in the older age group.
Bilateral vitreous cysts and asymptomatic posterior embryotoxon were coincidental findings which we noted on examination. We plan to follow up with the patient in order to monitor the cyst.
To conclude, bilateral pigmented free floating cysts are rare ocular malformations, and their association with posterior embryotoxon has so far not been reported in literature.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






