

Botulinum toxin type A (BTX-A) injection is the mainstay of management for patients with benign essential blepharospasm (BEB) owing to its proven safety and efficacy. BTX-A preparations available in various countries are Botox (Allergan, Irvine, CA, USA), Dysport (Ipsen, Slough, UK) [1,2,3], Xeomin (Merz Pharmaceuticals, Frankfurt am Main, Germany), and Prosigne (Lanzhou Biological Products, Lanzhou, China) [4,5]. Neuronox (Medytox, Seoul, Korea) is a recently introduced BTX-A preparation. Botox and Neuronox are purified extracts of BTX type A available as vacuum-dried and a freeze-dried lyophilized preparations, respectively [6,7]. Though both products are nearly similar, Neuronox is cheaper. This has a bearing on the choice of the product, especially for a repetitive disorder like BEB.
There are very limited data comparing the two products. Stone et al. [8] studied the dose-response relationship for inhibition of muscle force of Botox and Neuronox in a murine model and characterized the time course of recovery from the toxin-induced muscle paralysis. Gastrocnemius muscle force generation was examined following stimulation of the tibial nerve. Botox and Neuronox produced nearly equivalent decrements in muscle force (30% to 90%) at 4 days after toxin injection. At 28 days after injection (1 U/kg), muscle force had recovered from the effects of both toxin preparations. For facial spasms, only one double-blind, prospective, randomized control study has been conducted in humans to compare Botox and Neuronox in two separate cohorts of BEB patients in Korea [9]. The study concluded that both preparations are comparable in terms of their safety and efficacy. However, more studies are needed to consolidate the comparative data.
We therefore utilized the bilaterally symmetrical nature of BEB to conduct a split-face, prospective, randomized control study to compare safety and efficacy of the two BTX-A preparations in the management of BEB. A split face study eliminates any confounding factors that might be at play when two separate cohorts are studied.
Materials and Methods
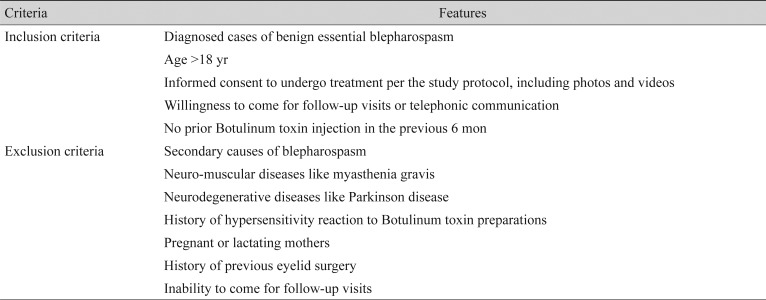
This split-face prospective randomized control study was conducted in accordance with the principles of the declaration of Helsinki. The study protocol as well as patient consent were approved by the institution review board of LV Prasad Eye Institute, Hyderabad, India (LEC 11-067). All patients consented to participation in the study before enrollment. The study was conducted at the LV Prasad Eye Institute, Hyderabad, India. All patients diagnosed with BEB and fulfilling the inclusion and exclusion criteria (Table 1) were included in this split-face study.
Since there was no prior split-face study to compare the two drugs, we decided to perform this as a pilot study enrolling a minimum of 20 patients. Each vial of Botox or Neuronox contained 100 units (U) of Clostridium Botulinum type A neurotoxin complex, 0.5 mg of human albumin, and 0.9 mg of sodium chloride in a sterile, dried solid without preservatives. Each 100-U vial was carefully reconstituted with 4 mL of sterile, non-preserved 0.9% normal saline to achieve a concentration of 2.5 U/0.1 mL. The reconstituted solution was stored in a refrigerator at 4Ōäā until needed. A 30-gauge half-inch needle was used for all injections after topical point-application of Prilocaine-Lidocaine cream. The study methodology was divided into the following three phases.
Pre-injection phase
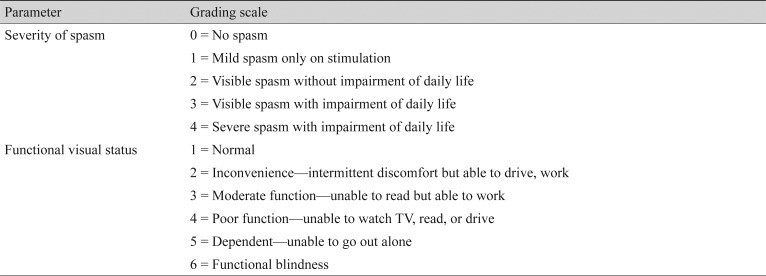
Written informed consent was obtained from the appropriately included participants. Severity of spasm and functional visual status were graded using the mentioned grading system (Table 2). The grading was done at the pre-injection visit and at subsequent follow-up assessments. Palpebral fissure height, lagophthalmos, and Schirmer's test without topical anaesthetic were documented at the pre-injection visit and at subsequent follow-up visits. Digital external photographs of the upper half of the face and a high-definition video clip were recorded to further document the measured parameters.
Injection phase
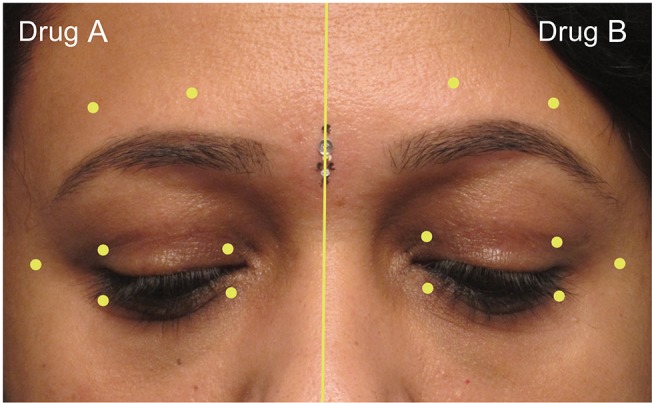
The injector was provided with two identical syringes containing equal amounts of toxin. To mask the identity of the toxin from the injector and the patient, the syringes were labeled as drug A and drug B. These syringes were loaded and provided to the injector by a single observer (MJA) who was blinded to the injection techniques and the post-injection evaluations. The right side of the face was injected first with either drug A or drug B, selected randomly by secret ballot method. An equal dose of the remaining drug was injected on the left side. All patients received 17.5 to 20 U of a given drug on each half side of the face. The identity of the drugs (drugs A and B) was concealed until the end of the statistical analysis. A standard technique was employed by a single injector (MNN) to inject 0.1 mL aliquots (2.5 U) per site with a 30-gauge needle over a Tuberculin syringe at seven prefixed sites in the periorbital area (Fig. 1). The sites were identical on both sides. The patients were prescribed preservative-free lubricant eye drops in both eyes.
Post-injection follow-up phase
At the 2- and 6-week post-injection follow-up visits, all the aforementioned clinical parameters were documented. Patients were encouraged to comply with follow-up visits by telephonic reminders. Objective outcome measures included improvement in the grades of severity of spasm and functional visual scale, as well as the occurrence of side effects like ptosis, lagophthalmos, and superficial punctuate keratitis.
Subjective outcome measures included duration of symptomatic relief, and a subjective feeling of a ŌĆśbetterŌĆÖ effect between the two sides of the face. To assess the latter, the patient was asked to choose which side (right or left) felt better than the other. Photographic and video graphic documentation was obtained at each follow-up visit. All the pre- and post-injection questionnaires and evaluations were performed by a single masked observer (SS).
Beyond the 6-week follow-up visit, patients were asked to report when the action of the toxin wore off, and they felt the need for the next injection. The patient was asked to report the subjective duration of the effect after complete washout of the action of the toxin, as well as any inequality in the effect between the two sides of the face.
Statistical analysis was performed using the SPSS ver. 16.0 (SPSS Inc., Chicago, IL, USA). For pre- and post-injection analysis, the paired t-test was used. For comparative analysis between drug A and drug B, independent t-tests were used.
Results
Twenty-four patients were enrolled in this prospective study. Fifteen were males, and nine females. The mean age was 52 years (SD, 11.1 years). The analysis of parameters such as severity of spasm, functional visual scale and forced choice of the better side was done considering the total number of patients as a denominator (n = 24) while for all other parameters, the denominator was taken as the total number of eyes (n = 48).
The most common presentation was involuntary closure of the eyes and/or increased rate of blinking noted in all patients. Two out of 24 patients also had spasmodic contractions of the lower face and neck region (lower facial dystonia), suggestive of Meige syndrome. The mean duration of the symptoms was 24.7 months.
Twenty-one patients received 17.5 U of the drug on each side (total 35 U), and three patients received 20 U (total 40 U). The identity of the drug was disclosed only after the statistical analysis was completed. Drug A was revealed to be Neuronox and drug B was Botox.
Five eyes had lagophthalmos ranging from 1 to 3 mm, and eight eyes had superficial punctuate keratopathy.
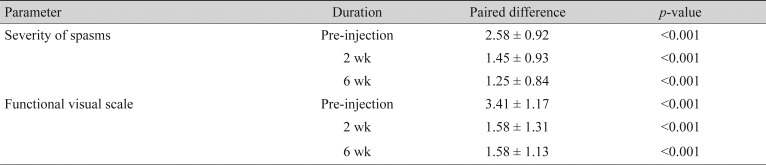
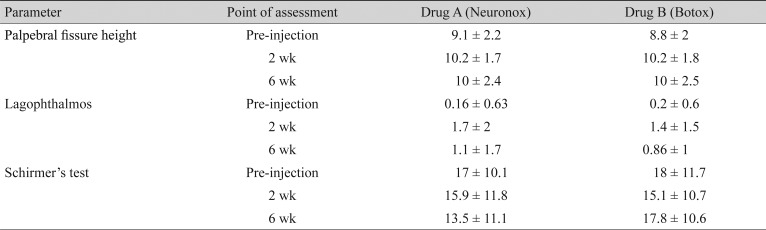
Among the objective outcome measures, the severity of spasm and the functional visual status showed statistically significant improvement (Table 3). Individual objective outcome measures like palpebral fissure height, induced lagophthalmos, and Schirmers test showed statistically significant differences, but the results were comparable in the Neuronox and Botox groups (Table 4).
At the 2- and 6-week follow-up, the difference in occurrence of superficial punctate keratopathy was not statistically significant in any of the groups.
Among the subjective outcome measures, the mean duration of the symptomatic relief was 3.8 months (SD, 1.6 months; range, 1 to 6 months). At the 2-week post-injection follow-up, all the patients showed symptomatic improvement. At the 2-week visit, three out of 24 (12.5%; 95% CI, 0 to 25.7) patients noted that the effect of the treatment was better on one side compared to the other, where the better side had received Neuronox. At the 6-week visit, one patient (4%) reported more activity on one half of the face compared to the other, where the better side had received Botox. These differences in their forced choice at 2 and 6 weeks were not statistically significant.
When asked to make a forced choice between the two sides about the benefit and the duration of the effect, all 24 patients felt that the effect of the treatment was similar on both sides of the face.
Discussion
Botulinum toxin type A is widely used in several specialties of medicine. It is used as the first-line treatment in the management of BEB. Botox is the oldest BTX-A preparation, and hence is time-tested and efficacious in the management of BEB. Neuronox is a recently introduced BTX-A preparation, and is structurally similar to Botox. The only difference between the two products is that Botox is a vacuum-dried preparation, whereas, Neuronox is a freeze-dried preparation.
Though animal studies have proven Neuronox to be effective and safe, only one study is available in the literature that compares it with Botox in humans. This study by Yoon et al. [9] compared the two preparations in two separate cohorts of patients of BEB, and found them to be comparable in safety and efficacy.
There are several merits to our study. We utilized the bilateral symmetric nature of BEB to conduct a split-face comparative study. In our study, all the participating patients received both preparations in a ŌĆśsplit-faceŌĆÖ manner on either side of the face. In our study, both the preparations were tested and compared in the same individuals, at the same time. We attempted to eliminate confounding factors related to intrinsic mechanisms, differences in the sensitivity to the drug, and genetic variability among different individuals, which could be potential causes of the differences in response to the drug. A single trained physician did the subjective assessment of the response to both the drugs.
The mean age at presentation and the chief presenting complaints in our study were similar to other reports. Half of our patients had received Botulinum toxin injection (Botox) in the past, and hence were well versed with its benefits and side effects. Following injection, there was a statistically significant improvement in the severity of spasm and the mean functional visual score. This indicates that both the drugs were equally effective. Among the subjective outcome measures, though the patients did report a difference between the two sides at the 2- and 6-week follow-up visit (three patients at 2 weeks reported that the Neuronox side was better, and one patient at 6 weeks reported that the Botox side was better), their final assessment at the conclusion of the toxin effect was that both sides were comparable.
The mean increase in palpebral fissure height, lagophthalmos (all eyes), and punctate keratopathy was significant in both groups. However, there were no statistically significant differences between the two when Botox was compared with Neuronox. This indicates that the side-effect profile was comparable for both drugs. This is expected, since the side-effect profile was directly comparable to the actual effect.
Our study is the first study to compare two Botulinum toxin products in a split-face manner. This avoids the inherent disadvantages of studying two drugs in two different cohorts of patients. The split-face study could be the best study model to compare two different drugs in the management of facial spasms.
In conclusion, our study indicates that Botox and Neuronox are equally effective in the management of BEB. The induced improvements in palpebral fissure height, visual impairment scale, and grade of severity of spasm are comparable. The side-effect profile (lagophthalmos and punctuate keratopathy) was also comparable.
 PDF Links
PDF Links PubReader
PubReader Full text via DOI
Full text via DOI Full text via PMC
Full text via PMC Download Citation
Download Citation Print
Print






